Need Assessment for Smartphone-Based Cardiac Telerehabilitation
- Affiliations
-
- 1Cardiac Wellness Center, Severance Hospital, Seoul, Korea.
- 2Cardiovascular Laboratory Part, Severance Hospital, Seoul, Korea.
- 3Division of Cardiology, Severance Cardiovascular Hospital and Cardiovascular Research Institute, Yonsei University College of Medicine, Seoul, Korea. smkang@yuhs.ac
- KMID: 2434543
- DOI: http://doi.org/10.4258/hir.2018.24.4.283
Abstract
OBJECTIVES
To identify the current status of smartphone usage and to describe the needs for smartphone-based cardiac telerehabilitation of cardiac patients.
METHODS
In 2016, a questionnaire survey was conducted in a supervised ambulatory cardiac rehabilitation (CR) program in a university affiliated hospital with the participation of heart failure or heart transplantation patients who were smartphone users. The questionnaire included questions regarding smartphone usage, demands for smartphone-based disease education, and home health monitoring systems. Results were described and analyzed according to principal diagnosis.
RESULTS
Ninety-six patients (66% male; mean age, 53 ± 11 years), including 56 heart failure and 40 heart transplantation patients, completed the survey (completion rate, 95%). The median daily smartphone usage time was 120 minutes (interquartile range, 60-300), and the most frequently used smartphone function was text messaging (61.5%). Of the patients, 26% stated that they searched for health-related information using their smartphones more than 1 time per week. The major source of health-related information was Internet browsing (50.0%), and the least sought source was the hospital's website (3.1%). Patients with heart failure expressed significantly higher needs for disease education on treatment plan, home health monitoring of blood pressure, and body weight (χ2 = 5.79, 6.27, 4.50, p < 0.05). Heart transplantation patients expressed a significant need for home health monitoring of body temperature (χ2 = 5.25, p < 0.05).
CONCLUSIONS
Heart failure and heart transplantation patients show high usage of and interest in mobile health technology. A smartphone-based cardiac telerehabilitation program should be developed based on high demand areas and modified to suit to each principal diagnosis.
Keyword
MeSH Terms
Figure
-

Figure 1 Needs for disease education through smartphone applications. The needs assessment of disease education through smartphone was conducted. HF patients expressed significantly higher needs for smartphone-based disease education for treatment plans (χ2 = 5.79, p < 0.05). HF: heart failure, HT: heart transplantation.
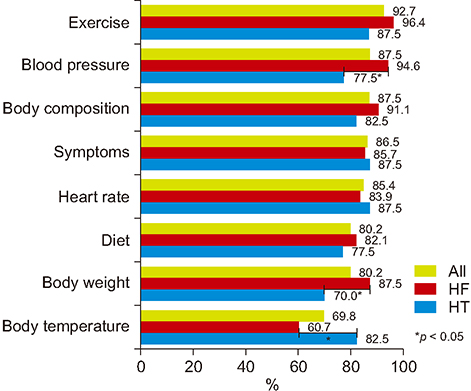
Figure 2 Needs for home health monitoring systems through smartphone applications. We identified the areas for which a home health monitoring system is needed through smartphone applications. Participants expressed significantly higher needs for home health monitoring of blood pressure and body weight in the HF group (χ2 = 6.27, 4.50, p < 0.05) and body temperature in the HT group (χ2 = 5.25, p < 0.05). HF: heart failure, HT: heart transplantation.
Reference
-
1. Taylor RS, Sagar VA, Davies EJ, Briscoe S, Coats AJ, Dalal H, et al. Exercise-based rehabilitation for heart failure. Cochrane Database Syst Rev. 2014; (4):CD003331.
Article2. Sandercock G, Hurtado V, Cardoso F. Changes in cardiorespiratory fitness in cardiac rehabilitation patients: a meta-analysis. Int J Cardiol. 2013; 167(3):894–902.
Article3. Balady GJ, Williams MA, Ades PA, Bittner V, Comoss P, Foody JM, et al. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: a scientific statement from the American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation. 2007; 115(20):2675–2682.
Article4. National Health Service in England. Commissioning guidance for rehabilitation [Internet]. London: NHS England;c2016. cited at 2018 Apr 13. Available from: https://www.england.nhs.uk/wp-content/uploads/2016/04/rehabilitation-comms-guid-16-17.pdf.5. Bjarnason-Wehrens B, McGee H, Zwisler AD, Piepoli MF, Benzer W, Schmid JP, et al. Cardiac rehabilitation in Europe: results from the European Cardiac Rehabilitation Inventory Survey. Eur J Cardiovasc Prev Rehabil. 2010; 17(4):410–418.
Article6. Martin AM, Woods CB. What sustains long-term adherence to structured physical activity after a cardiac event? J Aging Phys Act. 2012; 20(2):135–147.
Article7. Chow CK, Ariyarathna N, Islam SM, Thiagalingam A, Redfern J. mHealth in cardiovascular health care. Heart Lung Circ. 2016; 25(8):802–807.
Article8. Saner H. e-Cardiology and e-Health: from industry-driven technical progress to clinical application. Eur J Prev Cardiol. 2014; 21:2 Suppl. 2–3.
Article9. Yi JY, Kim Y, Cho YM, Kim H. Self-management of chronic conditions using mHealth interventions in Korea: a systematic review. Healthc Inform Res. 2018; 24(3):187–197.
Article10. World Health Organization. mHealth: new horizons for health through mobile technologies. Geneva, Switzerland: World Health Organization;2011.11. Pew Research Center. Mobile phone ownership over time [Internet]. Washington (DC): Pew Research Center;c2018. cited at 2018 May 22. Available from: http://www.pewinternet.org/fact-sheet/mobile/.12. Statista Inc. Smartphones industry: statistics and facts [Internet]. New York (NY): Statista Inc.;c2018. cited at 2018 may 5. Available from: https://www.statista.com/topics/840/smartphones/.13. Poushter J. Smartphone ownership rates skyrocket in many emerging economies, but digital divide remains [Internet]. Washington (DC): Pew Research Center;c2016. cited at 2018 May 5. Available from: http://www.pewglobal.org/2016/02/22/smartphone-ownership-rates-skyrocket-in-many-emerging-economies-but-digital-divide-remains/.14. Burke LE, Ma J, Azar KM, Bennett GG, Peterson ED, Zheng Y, et al. Current science on consumer use of mobile health for cardiovascular disease prevention: a scientific statement from the American Heart Association. Circulation. 2015; 132(12):1157–1213.
Article15. Han M, Lee E. Effectiveness of mobile health application use to improve health behavior changes: a systematic review of randomized controlled trials. Healthc Inform Res. 2018; 24(3):207–226.
Article16. Frederix I, Vanhees L, Dendale P, Goetschalckx K. A review of telerehabilitation for cardiac patients. J Telemed Telecare. 2015; 21(1):45–53.
Article17. Dale LP, Whittaker R, Eyles H, Mhurchu CN, Ball K, Smith N, et al. Cardiovascular disease self-management: pilot testing of an mHealth healthy eating program. J Pers Med. 2014; 4(1):88–101.
Article18. Buys R, Claes J, Walsh D, Cornelis N, Moran K, Budts W, et al. Cardiac patients show high interest in technology enabled cardiovascular rehabilitation. BMC Med Inform Decis Mak. 2016; 16:95.
Article19. Varnfield M, Karunanithi M, Lee CK, Honeyman E, Arnold D, Ding H, et al. Smartphone-based home care model improved use of cardiac rehabilitation in postmyocardial infarction patients: results from a randomized controlled trial. Heart. 2014; 100:1770–1779.
Article20. Lowres N, Neubeck L, Salkeld G, Krass I, McLachlan AJ, Redfern J, et al. Feasibility and cost-effectiveness of stroke prevention through community screening for atrial fibrillation using iPhone ECG in pharmacies: the SEARCH-AF study. Thromb Haemost. 2014; 111(6):1167–1176.
Article21. Redfern J, Usherwood T, Harris MF, Rodgers A, Hayman N, Panaretto K, et al. A randomised controlled trial of a consumer-focused e-health strategy for cardiovascular risk management in primary care: the Consumer Navigation of Electronic Cardiovascular Tools (CONNECT) study protocol. BMJ Open. 2014; 4(2):e004523.
Article22. Walsh JA 3rd, Topol EJ, Steinhubl SR. Novel wireless devices for cardiac monitoring. Circulation. 2014; 130(7):573–581.
Article23. Georgsson M, Staggers N. Quantifying usability: an evaluation of a diabetes mHealth system on effectiveness, efficiency, and satisfaction metrics with associated user characteristics. J Am Med Inform Assoc. 2016; 23(1):5–11.
Article24. mHealth Evidence by K4Health [Internet]. Baltimore (MD): mhealthevidence.org;c2016. cited at 2018 Apr 5. Available from: https://www.mhealthevidence.org/.25. Stoyanov SR, Hides L, Kavanagh DJ, Zelenko O, Tjondronegoro D, Mani M. Mobile app rating scale: a new tool for assessing the quality of health mobile apps. JMIR Mhealth Uhealth. 2015; 3(1):e27.
Article26. Korp P. Health on the Internet: implications for health promotion. Health Educ Res. 2006; 21(1):78–86.
Article27. Cleland JG, McDonagh T, Rigby AS, Yassin A, Whittaker T, Dargie HJ, et al. The national heart failure audit for England and Wales 2008–2009. Heart. 2011; 97(11):876–886.
Article28. Inglis SC, Clark RA, Dierckx R, Prieto-Merino D, Cleland JG. Structured telephone support or non-invasive telemonitoring for patients with heart failure. Cochrane Database Syst Rev. 2015; (10):CD007228.
Article29. Brocks Y, Zittermann A, Grisse D, Schmid-Ott G, Stock-Gieβendanner S, Schulz U, et al. Adherence of heart transplant recipients to prescribed medication and recommended lifestyle habits. Prog Transplant. 2017; 27(2):160–166.
Article30. Peterson JC, Allegrante JP, Pirraglia PA, Robbins L, Lane KP, Boschert KA, et al. Living with heart disease after angioplasty: a qualitative study of patients who have been successful or unsuccessful in multiple behavior change. Heart Lung. 2010; 39(2):105–115.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Correction: Need Assessment for Smartphone-Based Cardiac Telerehabilitation
- Literature Review of the Usefulness of Smartphone for the Evaluation and Treatment of Mental Disorders
- The Effect of Home-based Daily Journal Writing in Korean Adolescents with Smartphone Addiction
- A Pulmonary Telerehabilitation Program Improves Exercise Capacity and Quality of Life in Young Females Post-COVID-19 Patients
- The Relationship between Mother’s Smartphone Addiction and Children’s Smartphone Usage
