Twenty Years of Clinical Experience with Cardiac Myxomas: Diagnosis, Treatment, and Follow Up
- Affiliations
-
- 1Division of Cardiology, Hospital of the Government of the City of Buenos Aires Dr. Cosme Argerich, Buenos Aires, Argentina. tcianciulli@gmail.com
- 2Researchers of the Ministry of Health of the Government of the City of Buenos Aires, Buenos Aires, Argentina.
- KMID: 2433763
- DOI: http://doi.org/10.4250/jcvi.2019.27.e7
Abstract
- BACKGROUND
Cardiac myxomas are the most frequent cardiac tumors. Although histologically benign, in some cases myxomas may be lethal, due to impairment of cardiac dynamics and their thromboembolic potential. The study aimed to assess the clinical presentation of cardiac myxomas and their correlation with echocardiographic features and to describe the perioperative results and long-term outcome of surgically treated patients.
METHODS
A prospective study of 53 patients with cardiac myxomas who were operated the Hospital Argerich, followed clinically and with echocardiography from 1993 until 2013. All patients underwent echocardiographic studies.
RESULTS
The patient's mean age was 53 ± 16 years (62.3% were women). The most common findings were dyspnea followed by embolic events. Most tumors were localized in the left atrium (77.4%), mainly in the fossa ovalis (63%). Mean size of the tumors was 4.76 x 3.50 cm. Tumors were generally mobile (88%) and went beyond the valve plane, causing mild mitral or tricuspid valve obstruction (58%) and dilation of the respective atrial chamber. Patients whose tumors were obstructive had higher pulmonary artery systolic pressures (50 vs 33 mmHg p < 0.01). According to the echocardiographic appearance 67% of tumors had a smooth surface and the remaining 32% had a villous surface. All patients with embolic manifestations had tumors with a villous surface.
CONCLUSIONS
Clinical presentation relates to the ultrasound characteristics of myxomas. Smooth tumors are larger, occur with obstructive symptoms, and benefit from an elective surgery, whereas villous myxomas entailed a high embolic risk and require prompt surgical treatment.
Keyword
MeSH Terms
Figure
-

Figure 1 Smooth myxoma: surgical specimen (A), transesophageal echocardiogram (B). Villous myxoma: surgical specimen (C), transesophageal echocardiogram (D).

Figure 2 Biatrial villous myxoma (arrows). Transesophageal echocardiogram, 4-chamber view. LA: left atrium, LV: left ventricle, RA: right atrium, RV: right ventricle.
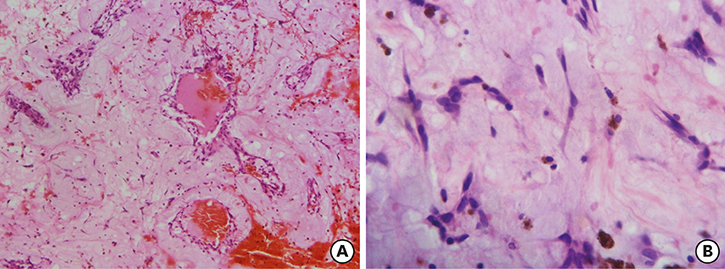
Figure 3 Histology of left atrial myxoma. Optic microscopy. (A) Hematoxylin–eosin stain. Proliferation of spindle and stellate mesenchymal cells around thin-walled vessels, with recent hemorrhage and macrophages filled with hemosiderin. Myxoid matrix with thin capillaries. (B) Microphotograph showing myxoid background, proliferation of star shaped cells, thin-walled vessels and macrophages with hemosiderin.

Figure 4 Left atrial myxoma with intra-tumor calcification. Transesophageal echocardiogram, 4-chamber view. The presence of calcification inside the tumor causes acoustic shadowing (arrow). LA: left atrium, LV: left ventricle, RA: right atrium, RV: right ventricle.
Cited by 2 articles
-
A Comprehensive Perspective of Clinical and Echocardiographic Features in the Differential Diagnosis of Cardiac Myxomas and Myxoma-Like Masses
Dong-Soo Kim
Korean Circ J. 2020;50(9):833-835. doi: 10.4070/kcj.2020.0309.Comparison of Clinical and Echocardiographic Characteristics between Cardiac Myxomas and Masses Mimicking Myxoma
Sun Hwa Lee, Joon Sung Park, Jae-Hyeong Park, Jung Yeon Chin, Won-Sik Yoon, Hyung Yoon Kim, Jae Yeong Cho, Kye Hun Kim, Won-Ho Kim
Korean Circ J. 2020;50(9):822-832. doi: 10.4070/kcj.2020.0024.
Reference
-
1. Suárez L, Cianciulli T. Tumores cardiacos. In : Bertolasi CA, Barrero C, Gimeno G, Liniado G, Mauro V, editors. Cardiologia 2000. 1st ed. Buenos Aires: Editorial Medica Panamericana;2000.2. Gošev I, Paić F, Durić Z, et al. Cardiac myxoma the great imitators: comprehensive histopathological and molecular approach. Int J Cardiol. 2013; 164:7–20.
Article3. Reynen K. Cardiac myxomas. N Engl J Med. 1995; 333:1610–1617.
Article4. Waller DA, Ettles DF, Saunders NR, Williams G. Recurrent cardiac myxoma: the surgical implications of two distinct groups of patients. Thorac Cardiovasc Surg. 1989; 37:226–230.
Article5. Wang Z, Chen S, Zhu M, et al. Risk prediction for emboli and recurrence of primary cardiac myxomas after resection. J Cardiothorac Surg. 2016; 11:22.
Article6. González EL, Pizzi M, Caponi MG, et al. Cardiac myxomas: clinical presentation, surgical outcomes and long-term prognosis. Rev Argent Cardiol. 2010; 78:108–113.7. Gabe ED, Rodríguez Correa C, Vigliano C, et al. Cardiac myxoma. Clinical-pathological correlation. Rev Esp Cardiol. 2002; 55:505–513.8. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015; 28:1–39.
Article9. Hahn RT, Abraham T, Adams MS, et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. 2013; 26:921–964.
Article10. Ha JW, Kang WC, Chung N, et al. Echocardiographic and morphologic characteristics of left atrial myxoma and their relation to systemic embolism. Am J Cardiol. 1999; 83:1579–1582.
Article11. Carney JA, Hruska LS, Beauchamp GD, Gordon H. Dominant inheritance of the complex of myxomas, spotty pigmentation, and endocrine overactivity. Mayo Clin Proc. 1986; 61:165–172.
Article12. Pinede L, Duhaut P, Loire R. Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases. Medicine (Baltimore). 2001; 80:159–172.13. Selkane C, Amahzoune B, Chavanis N, et al. Changing management of cardiac myxoma based on a series of 40 cases with long-term follow-up. Ann Thorac Surg. 2003; 76:1935–1938.
Article14. Kuroczyński W, Peivandi AA, Ewald P, Pruefer D, Heinemann M, Vahl CF. Cardiac myxomas: short- and long-term follow-up. Cardiol J. 2009; 16:447–454.15. Premaratne S, Hasaniya NW, Arakaki HY, Mugiishi MM, Mamiya RT, McNamara JJ. Atrial myxomas: experiences with 35 patients in Hawaii. Am J Surg. 1995; 169:600–603.
Article16. Kanda T, Umeyama S, Sasaki A, et al. Interleukin-6 and cardiac myxoma. Am J Cardiol. 1994; 74:965–967.
Article17. Mendoza CE, Rosado MF, Pacheco P. Interleukin-6 production and recurrent cardiac myxoma. J Thorac Cardiovasc Surg. 2001; 121:395–396.
Article18. Yokomuro H, Yoshihara K, Watanabe Y, Shiono N, Koyama N, Takanashi Y. The variations in the immunologic features and interleukin-6 levels for the surgical treatment of cardiac myxomas. Surg Today. 2007; 37:750–753.
Article19. Goswami KC, Shrivastava S, Bahl VK, Saxena A, Manchanda SC, Wasir HS. Cardiac myxomas: clinical and echocardiographic profile. Int J Cardiol. 1998; 63:251–259.
Article20. Craford C. Discussion of Glover R. The technique of mitral commisurotomy. In : In : Lam CR, editor. Cardiovascular surgery: studies in physiology, diagnosis and techniques. International Symposium on Cardiovascular Surgery; 1955 Mar; Henry Ford Hospital, Detroit. Philadelphia: Saunders;1955. 03.21. Garatti A, Nano G, Canziani A, et al. Surgical excision of cardiac myxomas: twenty years experience at a single institution. Ann Thorac Surg. 2012; 93:825–831.
Article22. Bortolotti U, Maraglino G, Rubino M, et al. Surgical excision of intracardiac myxomas: a 20-year follow-up. Ann Thorac Surg. 1990; 49:449–453.
Article23. Patil NP, Dutta N, Satyarthy S, Geelani MA, Kumar Satsangi D, Banerjee A. Cardiac myxomas: experience over one decade. J Card Surg. 2011; 26:355–359.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Carney Complex: Diagnosed 11 Years after Resection of Recurrent Cardiac Myxomas
- A Review of Cardiac Myxoma: 33-year Experience in a Single Institution
- Multi Modality Imaging Features of Cardiac Myxoma
- A Case of Multiple Right Atrial Myxomas with Pulmonary Embolism
- Primary Multiple Cardiac Myxomas in a Patient without the Carney Complex
