Prosthetic rehabilitation using an obturator in a fully edentulous patient who had partial maxillectomy
- Affiliations
-
- 1Divison of Prosthodontics, Department of Dentistry, Asan Medical Center, Seoul, Republic of Korea.
- 2Divison of Prosthodontics, Department of Dentistry, Asan Medical Center, College of Medicine, University of Ulsan, Seoul, Republic of Korea. ljhl11911@hanmail.net
- KMID: 2432370
- DOI: http://doi.org/10.14368/jdras.2018.34.4.331
Abstract
- Prosthetic rehabilitation of an edentulous patient who has a maxillary defect is difficult to achieve for many clinicians. The maxillary defect causes leakage of air during pronunciation and compromises denture stability, support and retention by reducing denture-bearing area and breaking peripheral seal. In these patients, the sizes and shapes of defects are very important factors which attribute to prognosis of maxillary obturators. This case report shows the prosthetic rehabilitation of the patient who had maxillectomy on the right maxillary sinus because of squamous cell carcinoma. The patient had a stepwise treatment protocol which started with pre-operative dental examination and followed by surgical, interim and definitive obturation phase. In this case, an acceptable level of retention could be obtained due to well-defined static defects and the preserved premaxillae and the patient was satisfied with the result of the treatment in the aspect of function and esthetics.
Keyword
MeSH Terms
Figure
-
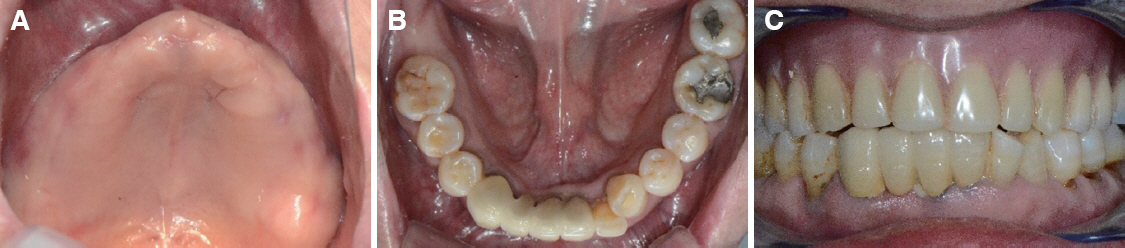
Fig. 1 Preoperative intraoral photographs. (A) Maxillary occlusal view, (B) Mandibular occlusal view, (C) Frontal view with old prostheses.

Fig. 2 Presurgical prosthetic planning. (A) Surgical margin on the study cast, (B) Centric relation record registration.
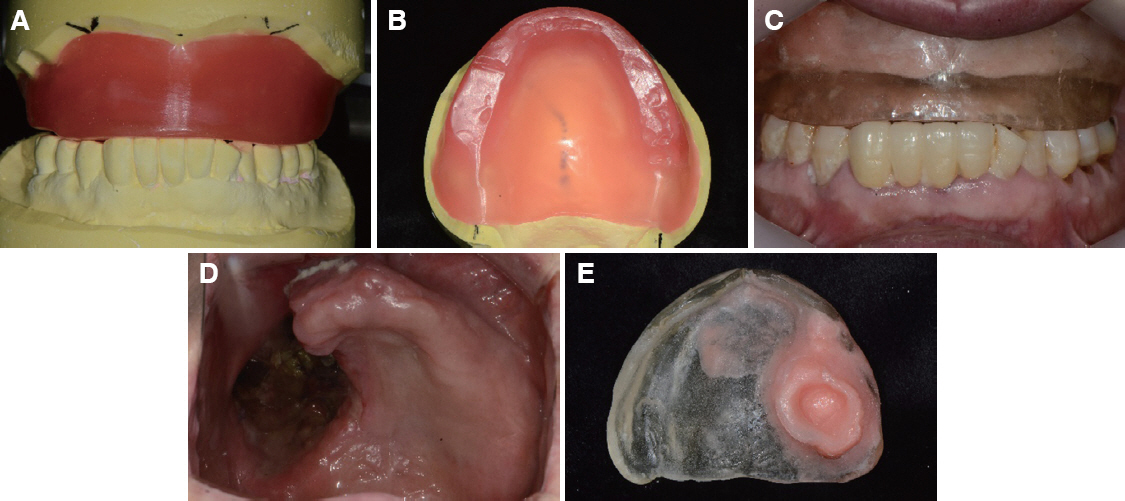
Fig. 3 Surgical obturation phase (A, B) Occlusal rim for surgical obturator, (C) Surgical obturator made of clear acrylic resin, (D) Maxillary occlusal view 2 weeks after maxillectomy, (E) Relined surgical obturator.

Fig. 4 Interim obturation phase. (A) Maxillary occlusal view 12 weeks after maxillectomy, (B) Modification of surgical obturator, (C) Intraoral photograph with modified surgical obturator.
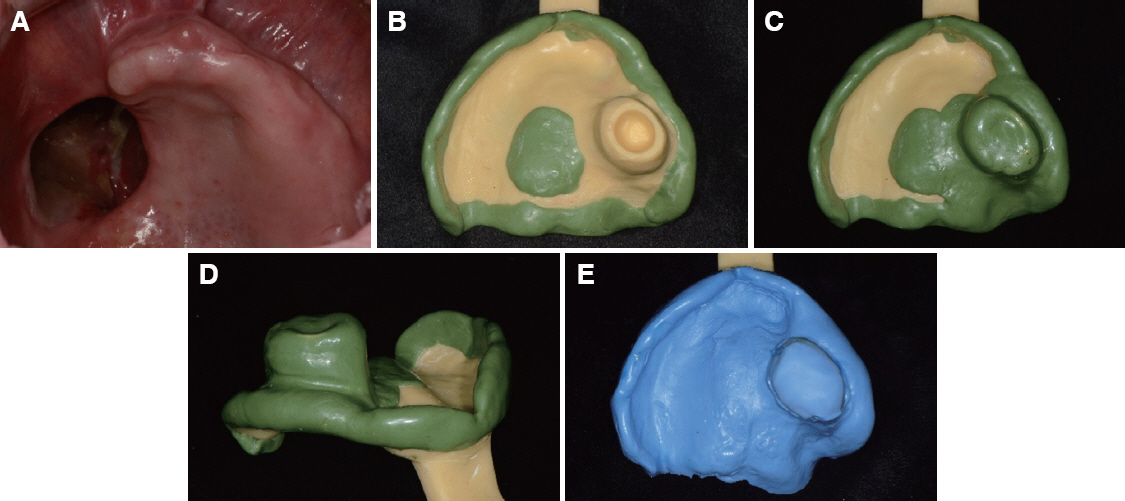
Fig. 5 Definitive obturation phase. (A) Maxillary occlusal view 16 weeks after maxillectomy, (B, C) Border molding of the definitive obturator, (D) Scar band presented on border molding compound wax, (E) Final impression completed with polyvinyl siloxane.

Fig. 6 (A) Mounting of the master cast, (B) Wax obturator, (C) Wash impression completed with light-body polyvinylsiloxane.
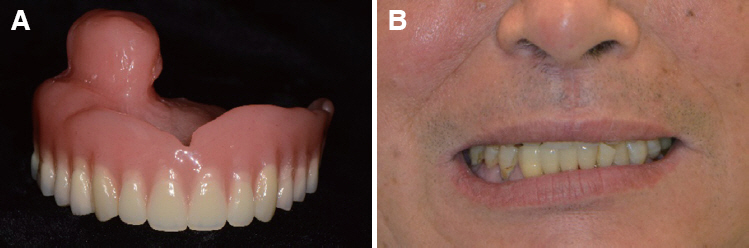
Fig. 7 (A) Definitive obturator, (B) Extraoral photograph after delivery of definitive obturator.
Reference
-
References
1. Oh WS, Roumanas E, Beumer J 3rd. Maxillofacial restoration after head and neck tumor therapy. Compend Contin Educ Dent. 2007; 28:70–6. PMID: 17319178.2. Beumer J 3rd, Marunick MT, Esposito SJ. Maxillofacial rehabilitation: prosthodontic and surgical management of cancer-related, acquired, and congenital defects of the head and neck. 3rd ed. Chicago: Quintessence Pub;2011. p. 155–212.3. Lang BR, Bruce RA. Presurgical maxillectomy prosthesis. J Prosthet Dent. 1967; 17:613–9. DOI: 10.1016/0022-3913(67)90133-3. PMID: 5298005.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prosthetic rehabilitation of a fully edentulous patient after maxillectomy: A case report
- Prosthetic rehabilitation of partially edentulous patient after maxillectomy: A case report
- Prosthetic rehabilitation by obturator considering the biomechanics in partially edentulous patient after maxillectomy
- Implant assisted obturator in patient after maxillectomy: a case report
- A three-dimensional finite element analysis of obturator prosthesis for edentulous maxilla
