Ann Rehabil Med.
2018 Apr;42(2):368-371. 10.5535/arm.2018.42.2.368.
Successful Management of Acquired Tracheomalacia of Patients With Amyotrophic Lateral Sclerosis: A Report of Three Cases
- Affiliations
-
- 1Department of Rehabilitation Medicine, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea. yjk5289@naver.com
- KMID: 2432210
- DOI: http://doi.org/10.5535/arm.2018.42.2.368
Abstract
- Tracheomalacia is characterized by weakness of the tracheal walls and supporting cartilage. It results in dynamic compression of the airway, where the cross-sectional area of the trachea is reduced by expiratory compression. Acquired tracheomalacia results from complications associated with the use of endotracheal or tracheostomy tubes. In this report, we present three cases of patients with amyotrophic lateral sclerosis (ALS) successfully treated for tracheomalacia, including one case where the patient underwent surgery for combined tracheoesophageal fistula. We discuss the appropriate management strategies for tracheomalacia in patients with ALS. Through these case reports, we note the results of ALS patients who will have tracheostomy, and who are therefore at risk of sustaining a long term high cuff pressure, this study provides an evaluation for tracheomalacia and therapeutic management which should be considered for improving patient care outcomes.
MeSH Terms
Figure
-
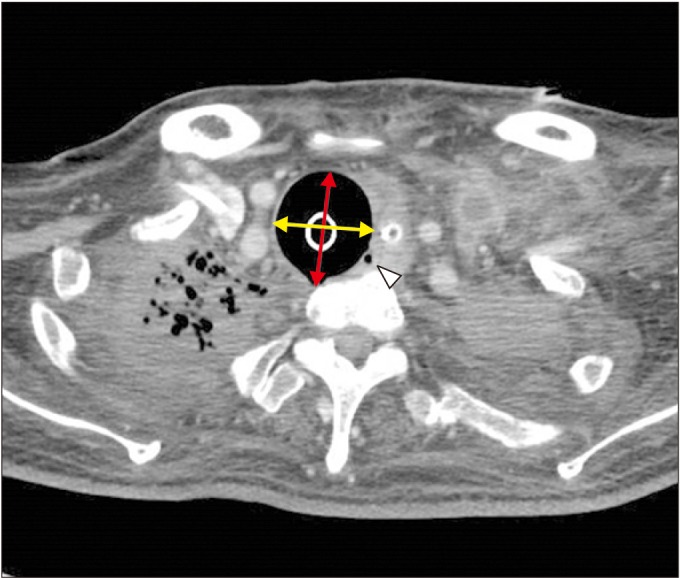
Fig. 1 Enlarged diameter of trachea (33.6 mm×37.5 mm) in inspiration computed tomography scan. A yellow arrow is a maximal transverse diameter (33.6 mm); red arrow, a maximal sagittal diameter (37.5 mm); white arrow head, tracheoesophageal fistula on tracheal level.
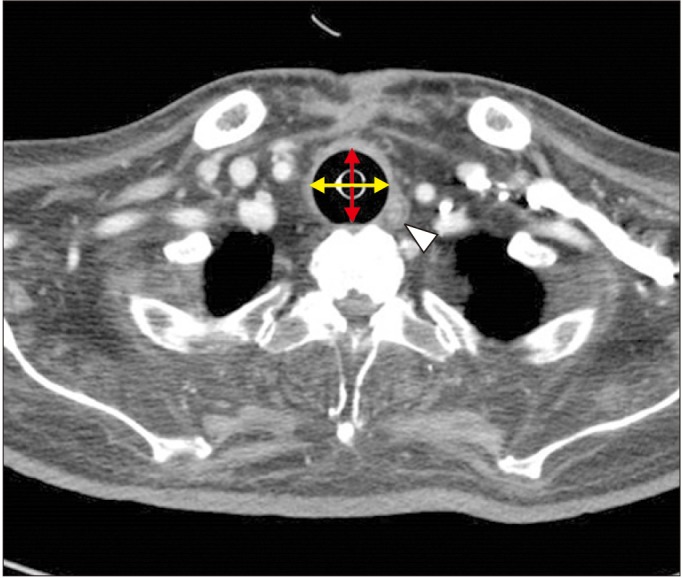
Fig. 2 Enlarged diameter of the trachea (28.66 mm×24.39 mm) with abscess formation and increase in soft tissue density at the posterior aspect of tracheostomy site in computed tomography view. A yellow arrow is a maximal transverse diameter (28.66 mm); red arrow, a maximal sagittal diameter (24.39 mm); white arrow head, abscess on tracheal level.
Reference
-
1. Reed MF, Mathisen DJ. Tracheoesophageal fistula. Chest Surg Clin N Am. 2003; 13:271–289. PMID: 12755313.
Article2. Jokinen K, Palva T, Sutinen S, Nuutinen J. Acquired tracheobronchomalacia. Ann Clin Res. 1977; 9:52–57. PMID: 883758.3. Feist JH, Johnson TH, Wilson RJ. Acquired tracheomalacia: etiology and differential diagnosis. Chest. 1975; 68:340–345. PMID: 169105.
Article4. Epstein PE. Radiologic diagnosis of diseases of the chest. Ann Intern Med. 2001; 135:1097.
Article5. Breatnach E, Abbott GC, Fraser RG. Dimensions of the normal human trachea. AJR Am J Roentgenol. 1984; 142:903–906. PMID: 6609569.
Article6. Flege JB. Tracheoesophageal fistula caused by cuffed tracheostomy tube. Ann Surg. 1967; 166:153–156. PMID: 6028837.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Syndrome of Progressive Bulbar Palsy in Amyotrophic Lateral Sclerosis: A Case Report
- Amyotrophic Lateral Sclerosis Associated With CADASIL
- Apraxia of Eyelid Closure and Motor Impersistence of Eyelid in a Patient with Amyotrophic Lateral Sclerosis
- A Case of Frontotemporal Dementia with Amyotrophic Lateral Sclerosis Presenting with Pathological Gambling
- Anesthetic management with neuromuscular monitoring and bispectral index in an amyotrophic lateral sclerosis patient: A case report
