Urogenit Tract Infect.
2018 Dec;13(3):79-83. 10.14777/uti.2018.13.3.79.
Patient's Factors Correlated with Prostate Volume Recovery after 5 Alpha Reductase Inhibitor Discontinuation
- Affiliations
-
- 1Department of Urology, National Police Hospital, Seoul, Korea. drmsk@korea.com
- KMID: 2431252
- DOI: http://doi.org/10.14777/uti.2018.13.3.79
Abstract
- PURPOSE
The 5 alpha reductase inhibitor (5ARI) reduces the size of the prostate and alleviates lower urinary tract symptoms. After stopping 5ARI, the prostate quickly recovers to its pre-medication size. The purpose of this study was to investigate the factors affecting the restoration of prostate size after 5ARI discontinuation.
MATERIALS AND METHODS
Between March 2009 and May 2017, patients who visited an outpatient clinic and were diagnosed with benign prostatic hyperplasia were selected and start 5ARI medication. After 6 months of medication, the patients stopped medication for 1 year. Meanwhile, we measured the prostate volumes of patients 3 times (before and after medication, after discontinuation) and divide the patients into 3 groups (maintained, intermediate, and restored) with recovered prostate volume ratio. After classification, we investigated the relationship between the variable factors (age, serum prostate-specific antigen, initial volume, reduced volume after medication) between groups.
RESULTS
Among the 147 selected patients, the mean age and plasma PSA level were 61.6±7.9 and 0.8±0.6, respectively. The mean initial prostate volume was 32.3±4.2 ml, which reduced to 23.2±3.2 ml after medication. After one year of discontinuation, the mean volume was 31.4±6.4 ml, with restoration to 101.5% of the reduced size. We noticed a tendency that patients with faster prostate volume recovery were generally older than those with slower recovery; however, this was not statistically significant. Other factors showed no relationship with prostate recovery.
CONCLUSIONS
When using 5ARI in elderly patients, continuous treatment seems better than intermittent treatment. If discontinuation is needed, short term follow-up is recommended.
MeSH Terms
Figure
-
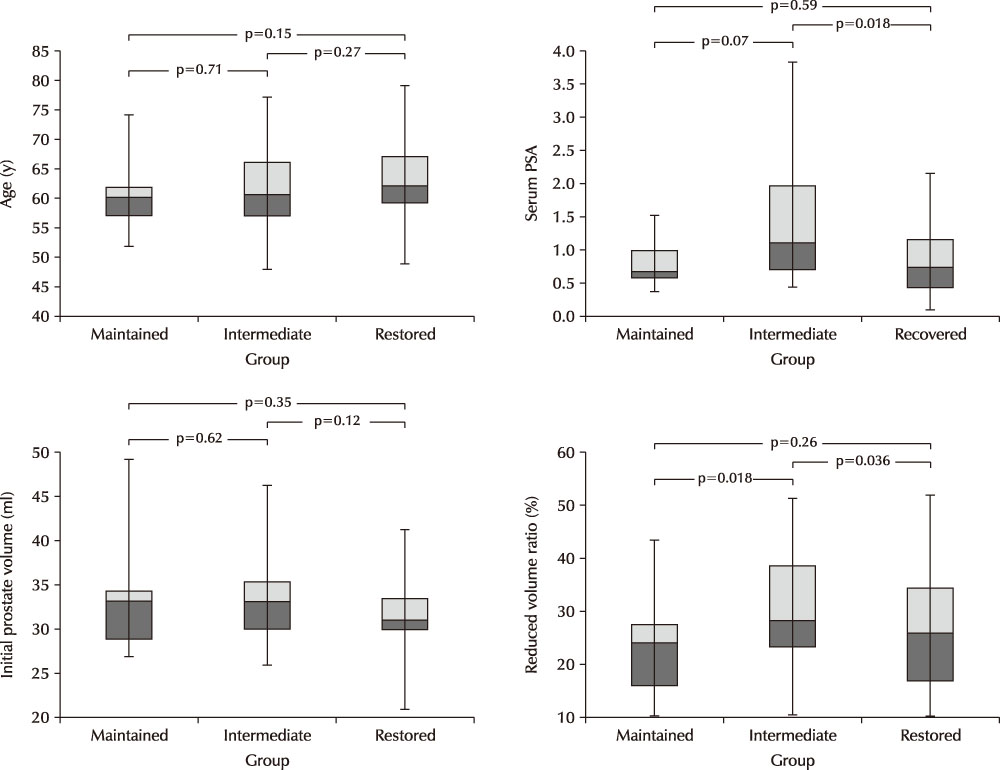
Fig. 1 Box plot for variable factors distribution in each groups and the results of t-tests. PSA: prostate-specific antigen.
Cited by 1 articles
-
Clinical Course of the Benign Prostate Hyplasia Patients during the Intermittent Use of 5-Alpha Reductase Inhibitors
Kwibok Choi, Byounghoon Kim, In-Chang Cho, Seung Ki Min
Urogenit Tract Infect. 2019;14(3):93-96. doi: 10.14777/uti.2019.14.3.93.
Reference
-
1. Emberton M, Andriole GL, de la Rosette J, Djavan B, Hoefner K, Vela Navarrete R, et al. Benign prostatic hyperplasia: a progressive disease of aging men. Urology. 2003; 61:267–273.
Article2. Kirby RS, Roehrborn C, Boyle P, Bartsch G, Jardin A, Cary MM, et al. Efficacy and tolerability of doxazosin and finasteride, alone or in combination, in treatment of symptomatic benign prostatic hyperplasia: the Prospective European Doxazosin and Combination Therapy (PREDICT) trial. Urology. 2003; 61:119–126.
Article3. Rigatti P, Brausi M, Scarpa RM, Porru D, Schumacher H, Rizzi CA. A comparison of the efficacy and tolerability of tamsulosin and finasteride in patients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia. Prostate Cancer Prostatic Dis. 2003; 6:315–323.
Article4. Traish AM, Mulgaonkar A, Giordano N. The dark side of 5a-Reductase inhibitors' therapy: sexual dysfunction, high Gleason grade prostate cancer and depression. Korean J Urol. 2014; 55:367–379.
Article5. Kim W, Jung JH, Kang TW, Song JM, Chung HC. Clinical effects of discontinuing 5-alpha reductase inhibitor in patients with benign prostatic hyperplasia. Korean J Urol. 2014; 55:52–56.
Article6. Roehrborn CG, Boyle P, Nickel JC, Hoefner K, Andriole G. ARIA3001 ARIA3002 and ARIA3003 Study Investigators. Efficacy and safety of a dual inhibitor of 5-alpha-reductase types 1 and 2 (dutasteride) in men with benign prostatic hyperplasia. Urology. 2002; 60:434–441.
Article7. Djavan B, Marberger M. A meta-analysis on the efficacy and tolerability of α1-adrenoceptor antagonists in patients with lower urinary tract symptoms suggestive of benign prostatic obstruction. Eur Urol. 1999; 36:1–13.
Article8. Kaplan SA, Lee JY, Meehan AG, Kusek JW. MTOPS Research Group. Long-term treatment with finasteride improves clinical progression of benign prostatic hyperplasia in men with an enlarged versus a smaller prostate: data from the MTOPS trial. J Urol. 2011; 185:1369–1373.
Article9. Traish AM. 5a-reductases in human physiology: an unfolding story. Endocr Pract. 2012; 18:965–975.10. Jun JEJ, Kinkade ATV, Tung ACH, Tejani AM. 5-alpha reductase inhibitors for treatment of benign prostatic hyperplasia: a systematic review and meta-analysis. Can J Hosp Pharm. 2017; 70:113–119.
Article11. Madersbacher S, Marszalek M, Lackner J, Berger P, Schatzl G. The long-term outcome of medical therapy for BPH. Eur Urol. 2007; 51:1522–1533.
Article12. Andersen JT, Nickel JC, Marshall VR, Schulman CC, Boyle P. Finasteride significantly reduces acute urinary retention and need for surgery in patients with symptomatic benign prostatic hyperplasia. Urology. 1997; 49:839–845.
Article13. Nickel JC, Fradet Y, Boake RC, Pommerville PJ, Perreault JP, Afridi SK, et al. Efficacy and safety of finasteride therapy for benign prostatic hyperplasia: results of a 2-year randomized controlled trial (the PROSPECT study). PROscar safety plus efficacy Canadian two year study. CMAJ. 1996; 155:1251–1259.14. Tenover JL, Pagano GA, Morton AS, Liss CL, Byrnes CA;. Efficacy and tolerability of finasteride in symptomatic benign prostatic hyperplasia: a primary care study. Clin Ther. 1997; 19:243–258.
Article15. Hudson PB, Boake R, Trachtenberg J, Romas NA, Rosenblatt S, Narayan P, et al. Efficacy of finasteride is maintained in patients with benign prostatic hyperplasia treated for 5 years. Urology. 1999; 53:690–695.
Article16. Rahimi-Ardabili B, Pourandarjani R, Habibollahi P, Mualeki A. Finasteride induced depression: a prospective study. BMC Clin Pharmacol. 2006; 6:7.
Article17. Descazeaud A, de La Taille A, Giuliano F, Desgrandchamps F, Doridot G. Negative effects on sexual function of medications for the treatment of lower urinary tract symptoms related to benign prostatic hyperplasia. Prog Urol. 2015; 25:115–127.18. Stoner E. The Finasteride Study Group. The clinical effects of a 5 alpha-reductase inhibitor, finasteride, on benign prostatic hyperplasia. J Urol. 1992; 147:1298–1302.
Article19. Jeong YB, Kwon KS, Kim SD, Kim HJ. Effect of discontinuation of 5alpha-reductase inhibitors on prostate volume and symptoms in men with BPH: a prospective study. Urology. 2009; 73:802–806.
Article20. Liaw YM, Kuo HC. Discontinuation of an alpha-1 blocker or 5-alpha-reductase inhibitor after combination medical treatment in patients with benign prostatic hyperplasia. Tzu Chi Med J. 2006; 18:91–96.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Effects of Discontinuing 5-Alpha Reductase Inhibitor in Patients With Benign Prostatic Hyperplasia
- Clinical Course of the Benign Prostate Hyplasia Patients during the Intermittent Use of 5-Alpha Reductase Inhibitors
- The Efficacy of Combination Therapy of 5 alpha -Reductase Inhibitor and of-Adrenergic Blocker in Benign Prostate Hyperplasia
- Significance of intraprostatic architecture and regrowth velocity for considering discontinuation of dutasteride after combination therapy with an alpha blocker: A prospective, pilot study
- The Change of Prostate-specific Antigen and Prostate-specific Antigen Density in Patients with Benign Prostatic Hyperplasia after Dutasteride Treatment
