Kosin Med J.
2018 Dec;33(2):240-244. 10.7180/kmj.2018.33.2.240.
A double-knotted pulmonary artery catheter with large loop in the right internal jugular vein: A case report
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Dong-A University College of Medicine, Busan, Korea. choisr@dau.ac.kr
- KMID: 2430741
- DOI: http://doi.org/10.7180/kmj.2018.33.2.240
Abstract
- Knotting of a pulmonary artery catheter (PAC) is a rare, but well-known complication of pulmonary artery (PA) catheterization. We report a case of a double-knotted PAC with a large loop in a patient with hepatocellular carcinoma (HCC) undergoing liver transplantation, which has been rarely reported in the literature. A PAC was advanced under pressure wave form guidance. PAC insertion was repeatedly attempted and the PAC was inserted 80 cm deep even though PAC should be normally inserted 45 to 55 cm deep. However, since no wave change was observed, we began deflating and pulling the balloon. At the 30-cm mark, the PAC could no longer be pulled. Fluoroscopy confirmed knotting of the PAC after surgery (The loop-formed PAC was shown in right internal jugular vein); thus, it was removed. For safe PA catheterization, deep insertion or repeated attempts should be avoided when the catheter cannot be easily inserted into the pulmonary artery. If possible, the insertion of PACs can be performed more safely by monitoring the movement of the catheter under fluoroscopy or transesophageal echocardiography.
MeSH Terms
Figure
-

Fig. 1 Fluoroscopy after the surgery shows a knotted pulmonary artery catheter with loop formation.
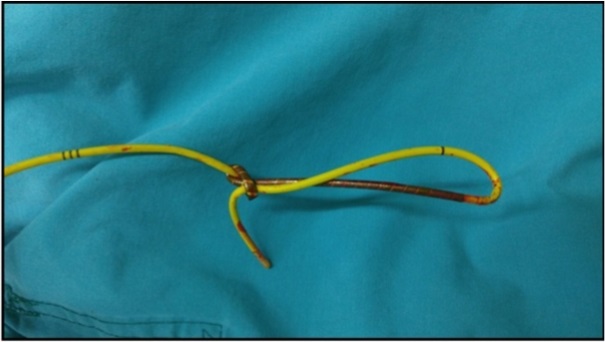
Fig. 2 Knotted pulmonary artery catheter removed by venotomy.
Reference
-
1. Swan HJ, Ganz W, Forrester J, Marcus H, Diamond G, Chonette D. Catheterization of the heart in man with use of a flow-directed balloon-tipped catheter. N Engl J Med. 1970; 283:447–451.
Article2. Lapinsky SE, Richards GA. Pro/con clinical debate: pulmonary artery catheters increase the morbidity and mortality of intensive care unit patients. Crit Care. 2003; 7:101–103.3. Hadian M, Kim HK, Severyn DA, Pinsky MR. Cross-comparison of cardiac output trending accuracy of LiDCO, PiCCO, FloTrac and pulmonary artery catheters. Crit Care. 2010; 14:R212.
Article4. Starzyk L, Yao E, Roche-Nagel G, Wasowicz M. Snaring swans: intraoperative knotting of pulmonary artery catheters. Anaesthesiol Intensive Ther. 2016; 48:66–70.
Article5. Evans DC, Doraiswamy VA, Prosciak MP, Silviera M, Seamon MJ, Rodriquez Funes VR, et al. Complications associcated with pulmonary artery catheters: a comprehensive clinical review. Scand J Surg. 2009; 98:199–208.
Article6. Colbert S, O'Hanlon DM, Quill DS, Keane P. Swan Ganz catheter--all in a knot. Eur J Anaesthesiol. 1997; 14:518–520.7. Böttiger BW, Schmidt H, Böhrer H, Martin E. Non-surgical removal of a knotted Swan-Ganz catheter. Anaesthesist. 1991; 40:682–686.8. Karanikas ID, Polychronidis A, Vrachatis A, Arvanitis DP, Simopoulos CE, Lazarides MK. Removal of knotted intravascular devices. Case report and review of the literature. Eur J Vasc Endovasc Surg. 2002; 23:189–194.
Article9. Georghiou GP, Vidne BA, Raanani E. Knotting of a pulmonary artery catheter in the superior vena cava: surgical removal and a word of caution. Heart. 2004; 90:e28.
Article10. Fibuch EE, Tuohy GF. Intracardiac knotting of a flow-directed balloon-tipped catheter. Anesth Analg. 1980; 59:217–212.11. Bossert T, Gummert JF, Bittner HB, Barten M, Walther T, Falk V, et al. Swan-Ganz catheter-induced severe complications in cardiac surgery: right ventricular perforation, knotting, and rupture of a pulmonary artery. J Card Surg. 2006; 21:292–295.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Upward Migration of Distal Ventriculoperitoneal Shunt Catheter into the Heart : Case Report
- A Case of Pulmonary Artery Catheter Malposition after the Weaning of Cardiopulmonary Bypass: A case report
- Uncommon Complications Related to Pulmonary Artery Catheterization (CCOmbo Swan-Ganz catheter): Two case report
- Intracardiac Knotting of a Balloon-tipped, Flow-directed Pulmonary Artery Catheter: A Case Report
- Surgical Removal of Knotted Pulmonary Artery Catheter: A Case Report
