Imaging and Clinical Data Distinguish Lymphadenopathy-First-Presenting Kawasaki Disease from Bacterial Cervical Lymphadenitis
- Affiliations
-
- 1Department of Pediatrics, Hallym University Sacred Heart Hospital, Anyang, Korea. rohetkim@yahoo.co.kr
- KMID: 2429999
- DOI: http://doi.org/10.4250/jcvi.2018.26.e29
Abstract
- BACKGROUND
Kawasaki disease (KD) sometimes presents with only fever and cervical lymphadenopathy before other clinical signs materialize. This lymphadenopathy-first-presenting Kawasaki disease (LKD) may be misdiagnosed as bacterial cervical lymphadenitis (BCL). We investigated characteristic imaging and clinical data for factors differentiating LKD from BCL.
METHODS
We compared imaging, clinical, and laboratory data of patients with KD and BCL. We included patients admitted to a single tertiary center between January 2015 and July 2018.
RESULTS
We evaluated data from 51 patients with LKD, 63 with BCL, and 218 with typical KD. Ultrasound imaging revealed multiple enlarged lymph nodes in both LKD and BCL patients. On the other hand, computed tomography (CT) showed more abscesses in patients with BCL. Patients with LKD were younger and showed higher systemic and hepatobiliary inflammatory markers and pyuria than BCL patients. In multivariable logistic regression, younger age and higher C-reactive protein (CRP) retained independent associations with LKD. A comparison of the echocardiographic findings in LKD and typical KD showed that patients with LKD did not have a higher incidence of coronary artery abnormalities (CAA).
CONCLUSIONS
LKD patients tend to have no abscesses on CT and more elevated systemic hepatobiliary inflammatory markers and pyuria compared to BCL patients. The absence of abscess on CT, younger age, and elevated CRP were the most significant variables differentiating LKD from BCL. There was no difference in CAA between LKD and typical KD.
MeSH Terms
Figure
-
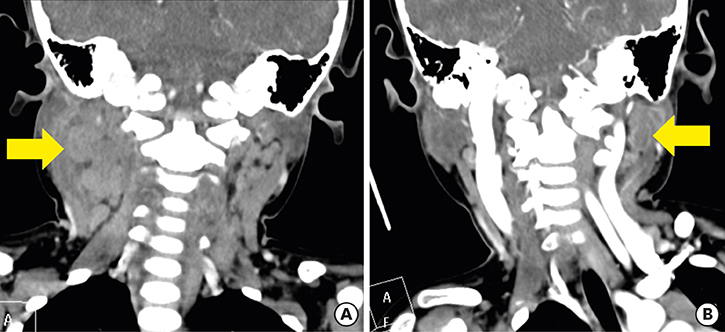
Figure 1 (A) Neck computed tomography image performed in a patient with lymphadenopathy-first-presenting Kawasaki disease; white arrow indicates multiple enlarged lymph nodes without abscess. (B) Neck computed tomography image performed in a patient with bacterial cervical lymphadenitis; white arrow indicates multiple enlarged lymph nodes with internal low density, suggesting abscess.
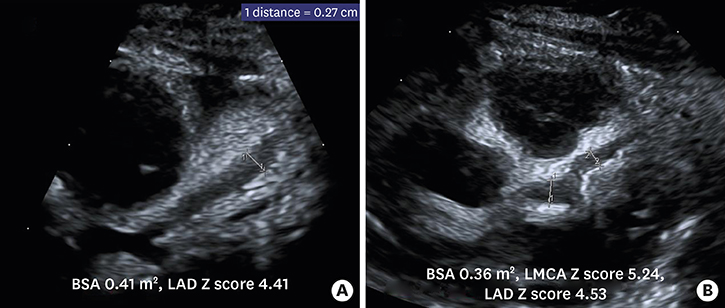
Figure 2 Echocardiographic images of a left coronary artery in parasternal short axis view. (A) In a patient with lymphadenopathy-first-presenting Kawasaki disease, the left coronary artery shows ectasia. (B) In a patient with typical Kawasaki disease, a marked dilated and tortuous coronary artery was revealed.
Cited by 2 articles
-
Diagnostic Applications for Clinical and Imaging Data in Kawasaki Disease with Lymphadenopathy-First-Presentation
Jae Sung Son
J Cardiovasc Imaging. 2018;26(4):247-249. doi: 10.4250/jcvi.2018.26.e32.Deep Neck Inflammation: Probable Kawasaki Disease in Korean Children
Sooyeon Lim, Na Young Lee, Seung Beom Han, Dae Chul Jeong, Jin Han Kang
Clin Exp Otorhinolaryngol. 2020;13(1):77-82. doi: 10.21053/ceo.2019.00948.
Reference
-
1. McCrindle BW, Rowley AH, Newburger JW, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017; 135:e927–99.
Article2. Wang CL, Wu YT, Liu CA, Kuo HC, Yang KD. Kawasaki disease: infection, immunity and genetics. Pediatr Infect Dis J. 2005; 24:998–1004.3. Nomura Y, Arata M, Koriyama C, et al. A severe form of Kawasaki disease presenting with only fever and cervical lymphadenopathy at admission. J Pediatr. 2010; 156:786–791.
Article4. Yanagi S, Nomura Y, Masuda K, et al. Early diagnosis of Kawasaki disease in patients with cervical lymphadenopathy. Pediatr Int. 2008; 50:179–183.
Article5. Kanegaye JT, Van Cott E, Tremoulet AH, et al. Lymph-node-first presentation of Kawasaki disease compared with bacterial cervical adenitis and typical Kawasaki disease. J Pediatr. 2013; 162:1259–1263.e2.
Article6. Kubota M, Usami I, Yamakawa M, Tomita Y, Haruta T. Kawasaki disease with lymphadenopathy and fever as sole initial manifestations. J Paediatr Child Health. 2008; 44:359–362.
Article7. Yun HW, Lee JY, Yang SI, et al. Comparison of cervical-lymph-node-first presentation of Kawasaki disease and typical Kawasaki disease. Pediatr Infect Vaccine. 2016; 23:10–17.
Article8. Jun WY, Ann YK, Kim JY, et al. Kawasaki disease with fever and cervical lymphadenopathy as the sole initial presentation. Korean Circ J. 2017; 47:107–114.
Article9. Waggoner-Fountain LA, Hayden GF, Hendley JO. Kawasaki syndrome masquerading as bacterial lymphadenitis. Clin Pediatr (Phila). 1995; 34:185–189.
Article10. Kao HT, Huang YC, Lin TY. Kawasaki disease presenting as cervical lymphadenitis or deep neck infection. Otolaryngol Head Neck Surg. 2001; 124:468–470.
Article11. Park AH, Batchra N, Rowley A, Hotaling A. Patterns of Kawasaki syndrome presentation. Int J Pediatr Otorhinolaryngol. 1997; 40:41–50.
Article12. Dallaire F, Dahdah N. New equations and a critical appraisal of coronary artery Z scores in healthy children. J Am Soc Echocardiogr. 2011; 24:60–74.
Article13. Roh K, Lee SW, Yoo J. CT analysis of retropharyngeal abnormality in Kawasaki disease. Korean J Radiol. 2011; 12:700–707.
Article14. Kato H, Kanematsu M, Kato Z, Teramoto T, Kondo N, Hoshi H. Computed tomographic findings of Kawasaki disease with cervical lymphadenopathy. J Comput Assist Tomogr. 2012; 36:138–142.
Article15. Tona R, Shinohara S, Fujiwara K, et al. Risk factors for retropharyngeal cellulitis in Kawasaki disease. Auris Nasus Larynx. 2014; 41:455–458.
Article16. Nozaki T, Morita Y, Hasegawa D, et al. Cervical ultrasound and computed tomography of Kawasaki disease: Comparison with lymphadenitis. Pediatr Int. 2016; 58:1146–1152.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Characteristics of Lymphadenopathy as the Initial Manifestation of Kawasaki Disease
- Etiologies and Clinical Characteristics of Cervical Lymphadenopathy in Children
- Kawasaki Disease Presenting as Cervical Lymphadenitis and Retropharyngeal Abscess
- Kawasaki disease presenting as retropharyngeal abscess
- CD68 Positive Histiocytic Necrotizing Lymphadenitis
