Gastric Tuberculosis Presenting as a Subepithelial Mass: A Rare Cause of Gastrointestinal Bleeding
- Affiliations
-
- 1Department of Radiology, Division of Gastroenterology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea.
- 2Department of Internal Medicine, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea. endoksj@gmail.com
- 3Department of Surgery, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea.
- KMID: 2429947
- DOI: http://doi.org/10.4166/kjg.2018.72.6.304
Abstract
- Gastric tuberculosis accounts for approximately 2% of all cases of gastrointestinal tuberculosis. Diagnosis of gastric tuberculosis is challenging because it can present with various clinical, endoscopic, and radiologic features. Tuberculosis manifesting as a gastric subepithelial tumor is exceedingly rare; only several dozen cases have been reported. A 30-year-old male visited emergency room of our hospital with hematemesis and melena. Abdominal CT revealed a 2.5 cm mass in the gastric antrum, and endoscopy revealed a subepithelial mass with a visible vessel at its center on gastric antrum. Primary gastric tuberculosis was diagnosed by surgical wedge resection. We report a rare case of gastric tuberculosis mimicking a subepithelial tumor with acute gastric ulcer bleeding.
MeSH Terms
Figure
-
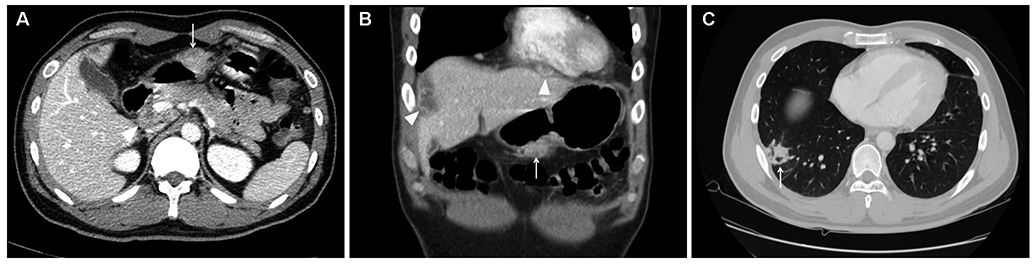
Fig. 1 (A) Axial contrast-enhanced CT image revealed a relatively well-defined soft tissue mass (arrow) on the anterior wall of antrum and an enlarged lymph node with peripheral rim enhancement and a hypodense center (arrowhead) in the periportal area. (B) Coronal reformatted contrast-enhanced CT scan showing low attenuating masses with thickened walls (arrowheads) in both subphrenic spaces and an exophytic, enhancing mass in gastric antrum (arrow). (C) CT images taken with lung window setting showing airspace consolidation (arrow) in the right lower lobe. CT, computed tomography.
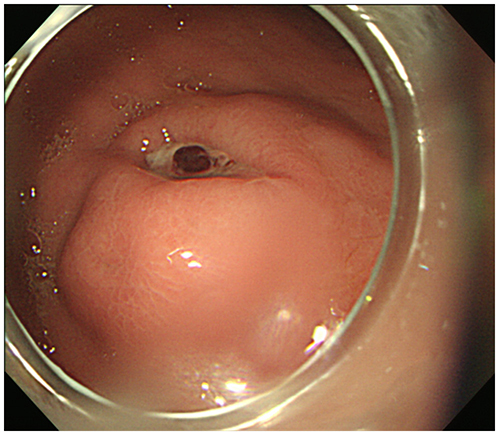
Fig. 2 Gastroduodenal endoscopy revealed an intraluminal protruding mass lesion with overlying ulceration and a visible vessel in the anterior wall of gastric antrum.
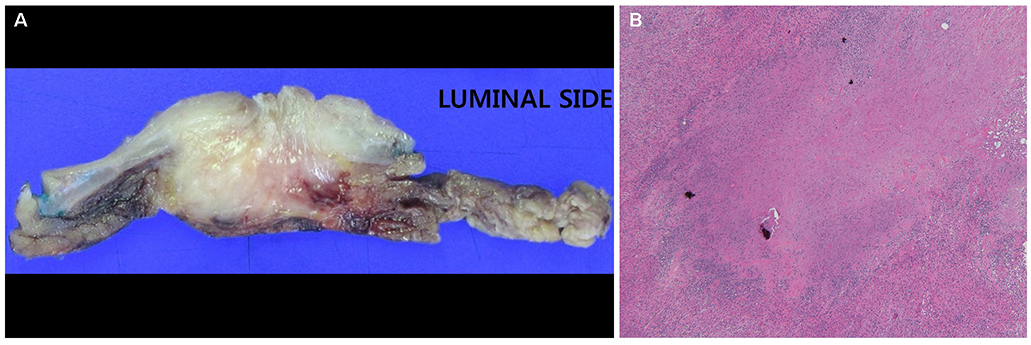
Fig. 3 (A) The cut surface of the gross specimen showed a pale white, well-circumscribed mass with ulceration in the stomach antrum. (B) Histopathologic examination demonstrated chronic granulomatous inflammation with caseous necrosis surrounded by inflammatory cells (H&E, ×40).
Reference
-
1. Singh V, Jain AK, Agrawal AK, et al. Clinicopathological profile of abdominal tuberculosis. Br J Clin Pract. 1995; 49:22–24.2. Subei I, Attar B, Schmitt G, Levendoglu H. Primary gastric tuberculosis: a case report and literature review. Am J Gastroenterol. 1987; 82:769–772.3. Petroianni A, Mugnaini L, Laurendi G, et al. Abdominal tuberculosis mimicking Crohn's disease: a difficult diagnosis. Report of a case. Panminerva Med. 2002; 44:155–158.4. Talukdar R, Khanna S, Saikia N, Vij JC. Gastric tuberculosis presenting as linitis plastica: a case report and review of the literature. Eur J Gastroenterol Hepatol. 2006; 18:299–303.
Article5. Rana SS, Bhasin DK, Srinivasan R, Singh K. Gastric outlet obstruction caused by tuberculosis and diagnosed by endoscopic ultrasound-guided fine needle aspiration. Endoscopy. 2011; 43:Suppl 2 UCTN. E117–E118.
Article6. Kim SH, Park JH, Kang KH, et al. Gastric tuberculosis presenting as a submucosal tumor. Gastrointest Endosc. 2005; 61:319–322.
Article7. Gupta V, Goel MM, Noushif M, Rai P, Gupta P, Chandra A. Primary gastric tuberculosis mimicking gastrointestinal stromal tumor. Am J Gastroenterol. 2012; 107:1269–1270.
Article8. Ardengh JC, Vaiciunas S, Kemp R, Venco F, Lima-Filho ER, dos Santos JS. Upper endoscopy versus endosonography in differential diagnosis of gastrointestinal bulging. Arq Gastroenterol. 2011; 48:236–241.
Article9. Kruijshaar ME, Abubakar I. Increase in extrapulmonary tuberculosis in England and Wales 1999–2006. Thorax. 2009; 64:1090–1095.
Article10. Tromba JL, Inglese R, Rieders B, Todaro R. Primary gastric tuberculosis presenting as pyloric outlet obstruction. Am J Gastroenterol. 1991; 86:1820–1822.11. Mitchell RS, Bristol LJ. Intestinal tuberculosis: an analysis of 346 cases diagnosed by routine intestinal radiography on 5,529 admissions for pulmonary tuberculosis, 1924–49. Am J Med Sci. 1954; 227:241–249.12. Shibagaki K, Miyaike J, Onji M, et al. Submucosal tumor-like lesion originating from colon tuberculosis: a case report and review of the literature. Clin J Gastroenterol. 2015; 8:207–211.
Article13. Kim DY, Bang S, Park BK, et al. Tuberculous mesenteric lymphadenitis involving the gastric wall: case report. Gastrointest Endosc. 2005; 62:799–802.
Article14. Lee TH, Cho JY, Bok GH, Cho WY, Jin SY. Intra-abdominal tuberculous lymphadenitis diagnosed using an endoscopic ultrasonography-guided Procore needle biopsy. Clin Endosc. 2013; 46:77–80.
Article15. Paustian FF, Marshall JB. Intestinal tuberculosis. In : Berk JE, editor. Gastroenteroscopy. Volume 3. 4th ed. Philadelphia: WB Saunders;1985. p. 2018–2036.16. Gaines W, Steinbach HL, Lowenhaupt E. Tuberculosis of the stomach. Radiology. 1952; 58:808–819.
Article17. Rao YG, Pande GK, Sahni P, Chattopadhyay TK. Gastroduodenal tuberculosis management guidelines, based on a large experience and a review of the literature. Can J Surg. 2004; 47:364–368.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Gastric Calcifying Fibrous Tumor Presenting as a Subepithelial Tumor
- Incidental Gastrointestinal Subepithelial Mass
- Gastric Ulcer Bleeding associated with a Left Gastric Artery Pseudoaneurysm
- A Case of Gastric Candidiasis Presented as Subepithelial Mass in an Immunocompromised Host
- Diagnosis of Gastric Subepithelial Tumor: Focusing on Endoscopic Ultrasonography
