World J Mens Health.
2019 Jan;37(1):93-98. 10.5534/wjmh.180047.
Elevated Body Mass Index Is Associated with Secondary Hypogonadism among Men Presenting to a Tertiary Academic Medical Center
- Affiliations
-
- 1Department of Urology, University of Miami Miller School of Medicine, Miami, FL, USA. jmm557@med.miami.edu
- 2Division of Endocrinology, Department of Medicine, University of Miami Miller School of Medicine, Miami, FL, USA.
- KMID: 2429726
- DOI: http://doi.org/10.5534/wjmh.180047
Abstract
- PURPOSE
To characterize the population of hypogonadal men who presented to a tertiary academic urology clinic and evaluate risk factors for primary vs. secondary hypogonadism.
MATERIALS AND METHODS
We evaluated all men with International Classification of Diseases-9 diagnosis codes R68.82 and 799.81 for low libido, 257.2 for testicular hypofunction, and E29.1 for other testicular hypofunction at a tertiary academic medical center from 2013 to 2017. We included men who had testosterone (T) and luteinizing hormone (LH) drawn on the same day. We classified men based on T and LH levels into eugonadal, primary, secondary, and compensated hypogonadism. Risk factors including age, body mass index (BMI) over 30 kg/m2, current smoking status, alcohol use greater than 5 days per week, and Charlson comorbidity index greater than or equal to 1 were investigated and measured in each group using the eugonadal group for reference.
RESULTS
Among the 231 men who had both T and LH levels, 7.4%, 42.4%, and 7.4% were classified as primary, secondary, and compensated hypogonadism, respectively. Only elevated BMI was associated with secondary hypogonadism compared to eugonadal men (median BMI, 30.93 kg/m2 vs. 27.69 kg/m2, p=0.003). BMI, age, comorbidities, smoking, or alcohol use did not appear to predict diagnosis of secondary hypogonadism.
CONCLUSIONS
Secondary hypogonadism appears to be the most common cause of hypogonadism among men complaining of low T and decreased libido at a tertiary academic medical center. Secondary hypogonadism is associated with elevated BMI and therefore obesity should be used as a marker to evaluate men for both T and LH levels.
Keyword
MeSH Terms
Figure
-
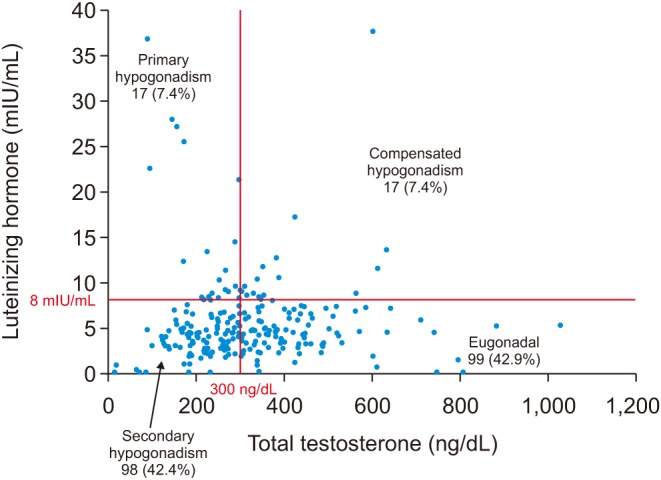
Fig. 1 Of the 231 men included in our study population, 99 (42.9%) were eugonadal, 98 (42.4%) had secondary hypogonadism, 17 (7.4%) had primary hypogonadism, and 17 (7.4%) had compensated hypogonadism.
Reference
-
1. Bhasin S, Cunningham GR, Hayes FJ, Matsumoto AM, Snyder PJ, Swerdloff RS, et al. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010; 95:2536–2559. PMID: 20525905.
Article2. Mulhall JP, Trost LW, Brannigan RE, Kurtz EG, Redmon JB, Chiles KA, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J Urol. 2018; 200:423–432. PMID: 29601923.
Article3. Heidelbaugh JJ. Endocrinology update: testicular hypogonadism. FP Essent. 2016; 451:31–41. PMID: 27936533.4. Tajar A, Forti G, O'Neill TW, Lee DM, Silman AJ, Finn JD, et al. Characteristics of secondary, primary, and compensated hypogonadism in aging men: evidence from the European Male Ageing Study. J Clin Endocrinol Metab. 2010; 95:1810–1818. PMID: 20173018.
Article5. Ramasamy R, Scovell JM, Kovac JR, Lipshultz LI. Testosterone supplementation versus clomiphene citrate for hypogonadism: an age matched comparison of satisfaction and efficacy. J Urol. 2014; 192:875–879. PMID: 24657837.
Article6. Mulligan T, Frick MF, Zuraw QC, Stemhagen A, McWhirter C. Prevalence of hypogonadism in males aged at least 45 years: the HIM study. Int J Clin Pract. 2006; 60:762–769. PMID: 16846397.7. Tajar A, Forti G, O'Neill TW, Lee DM, Silman AJ, Finn JD, et al. Characteristics of secondary, primary, and compensated hypogonadism in aging men: evidence from the European Male Ageing Study. J Clin Endocrinol Metab. 2010; 95:1810–1818. PMID: 20173018.
Article8. Traish AM, Guay A, Feeley R, Saad F. The dark side of testosterone deficiency: I. Metabolic syndrome and erectile dysfunction. J Androl. 2009; 30:10–22. PMID: 18641413.
Article9. Porte D Jr, Baskin DG, Schwartz MW. Insulin signaling in the central nervous system: a critical role in metabolic homeostasis and disease from C. elegans to humans. Diabetes. 2005; 54:1264–1276. PMID: 15855309.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Low Serum Testosterone Concentrations in Hospitalized Men with Poorly Controlled Type 2 Diabetes
- Difference of the Obesity Index, Blood Pressure and Serum Lipids in Abdominal and Non Abdominal in Men and Women
- Effectiveness Of Measurement Of Serum Testosterone Concentration As Screening Test In Impotent Men
- The relationship between the development of musculoskeletal disorders, body mass index, and academic stress in Bahraini University students
- Cross-Sectional Association of Metabolic Syndrome and Its Components with Serum Testosterone Levels in a Korean-Screened Population
