One-stage Hip Reconstruction for Developmental Hip Dysplasia in Children over 8 Years of Age
- Affiliations
-
- 1Department of Orthopaedic and Spine Surgery, Ghurki Trust Teaching Hospital, Lahore, Pakistan. irfanqadir88@gmail.com
- KMID: 2427930
- DOI: http://doi.org/10.5371/hp.2018.30.4.260
Abstract
- PURPOSE
This study was performed to assess the clinical and radiological outcomes following one-stage hip reconstruction, consisting of open reduction femoral shortening and pelvic osteotomy, for neglected developmental dislocation of the hip (DDH).
MATERIALS AND METHODS
This is a retrospective analysis of 77 hips in 65 patients (46 females and 19 males; 12 had bilateral dislocations), operated at a Ghurki Trust Teaching Hospital in Pakistan between 2013 and 2015. The average age at surgery was 11.02±3.43 years. According to the Tönnis classification, there were 10, 14, 22, and 31 patients in grades 1, 2, 3, and 4, respectively. The pelvic procedure utilized in this study was triple osteotomy (47 hips) followed by double and Salter osteotomy (18 and 12 hips, respectively). Postoperative evaluations were conducted using the modified MacKay's scoring system (functional outcomes) and Severin's scoring method (radiological assessment).
RESULTS
Postoperatively, there were 38 (49.4%), 19 (24.7%), 14 (18.2%), and 6 (7.8%) hips in Severin grade I, II, III and IV, respectively. According to the modified McKay criteria, there were 22 hips (28.6%) in excellent condition, 44 (57.1%) in good condition, 9 (11.7%) in fair condition and 2 (2.6%) in poor condition. Both patients with poor outcomes had an unstable, painful hip with evidence of avascular necrosis of the femoral head.
CONCLUSION
Based on the results presented here, we recommend the single stage procedure of open reduction, femoral shortening and pelvic osteotomy for treatment of DDH in older children with good to excellent functional and radiological outcomes.
MeSH Terms
Figure
-
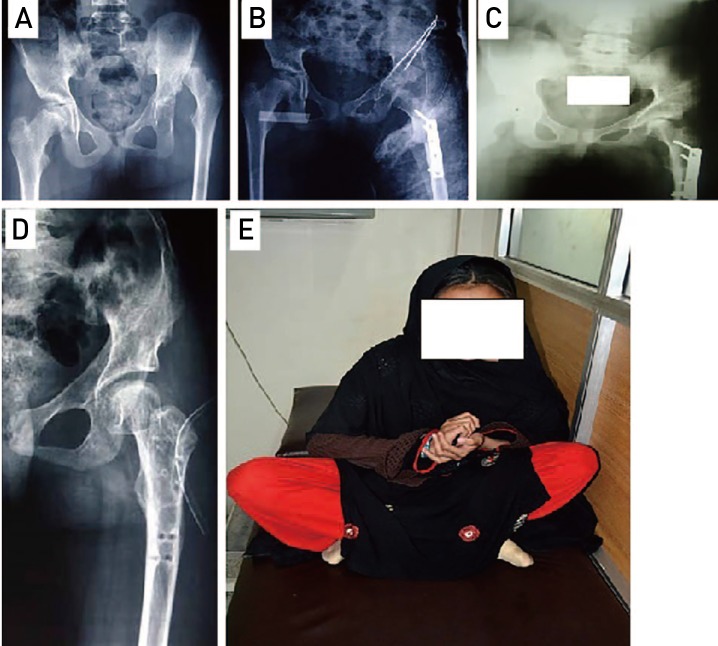
Fig. 1 Case presentation of a 10 year-old female with neglected developmental dysplasia of hip (DDH). (A) Preoperative X-ray showing left side Tönnis grade 4 DDH. (B) Immediate postoperative X-ray after open reduction, femoral shortening and triple pelvic osteotomy. (C) The follow-up X-ray after 6 months. (D) The follow-up X-ray after 2 years revealing congruent hip joint without evidence of avascular necrosis in femoral head. (E) Clinical picture illustrating patient's ability to squat.
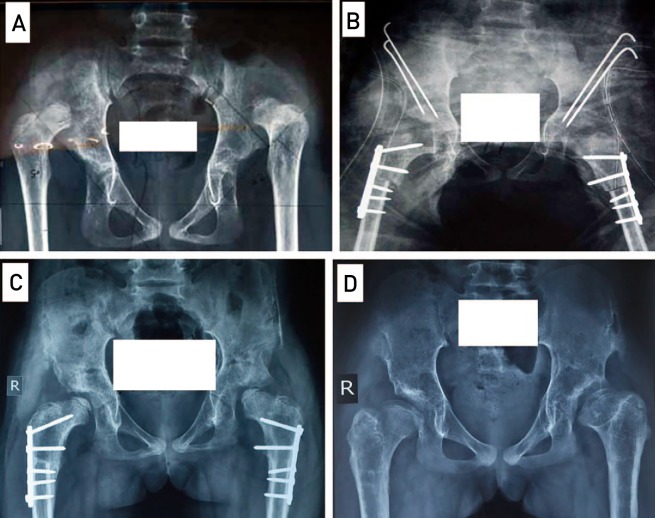
Fig. 2 Case presentation of an 11 year-old female with neglected developmental dysplasia of hip (DDH). (A) Preoperative X-ray showing bilateral Tönnis grade 4 DDH. (B) Immediate postoperative X-ray after bilateral open reduction, femoral shortening and Salter osteotomy on right side and double pelvic osteotomy on left side. (C) The follow-up X-ray after 1 year. (D) The follow up X-ray after removal of femur plates showing congruent hip joint bilaterally after two year. However, there is evidence of avascular necrosis in femur head on left side.
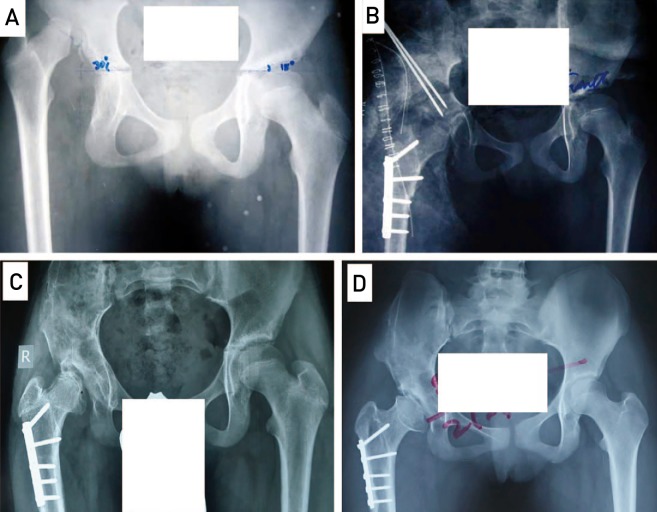
Fig. 3 Case presentation of 12 year-old female with neglected developmental dysplasia of hip (DDH). (A) Preoperative X-ray shows Tönnis grade 4 DDH on the right side. (B) Immediate postoperative X-ray after open reduction, femoral shortening and Salter osteotomy. (C) The follow-up X-ray after 1 year. (D) The follow-up X-ray after 2 years showing congruent hip joint with evidence of avascular necrosis in femur head.
Reference
-
1. Yagmurlu MF, Bayhan IA, Tuhanioglu U, Kilinc AS, Karakas ES. Clinical and radiological outcomes are correlated with the age of the child in single-stage surgical treatment of developmental dysplasia of the hip. Acta Orthop Belg. 2013; 79:159–165. PMID: 23821967.2. Vallamshetla VR, Mughal E, O'Hara JN. Congenital dislocation of the hip. A re-appraisal of the upper age limit for treatment. J Bone Joint Surg Br. 2006; 88:1076–1081. PMID: 16877609.3. Ok IY, Kim SJ, Ok JH. Operative treatment of developmental hip dysplasia in children aged over 8 years. J Pediatr Orthop B. 2007; 16:256–261. PMID: 17527102.
Article4. Papavasiliou VA, Papavasiliou AV. Surgical treatment of developmental dysplasia of the hip in the periadolescent period. J Orthop Sci. 2005; 10:15–21. PMID: 15666117.
Article5. Ashley RK, Larsen LJ, James PM. Reduction of dislocation of the hip in older children: a preliminary report. J Bone Joint Surg Am. 1972; 54:545–550. PMID: 5055152.6. El-Tayeby HM. One-stage hip reconstruction in late neglected developmental dysplasia of the hip presenting in children above 8 years of age. J Child Orthop. 2009; 3:11–20. PMID: 19308607.
Article7. Shih CH, Shih HN. One-stage combined operation of congenital dislocation of the hips in older children. J Pediatr Orthop. 1988; 8:535–539. PMID: 3170731.
Article8. McKay DW. A comparison of the innominate and the pericapsular osteotomy in the treatment of congenital dislocation of the hip. Clin Orthop Relat Res. 1974; (98):124–132. PMID: 4817221.
Article9. Tönnis D. Congenital hip dislocation. Avascular necrosis. New York: Thieme-Stratton;1982.10. Severin E. Contribution to the knowledge of congenital dislocation of the hip joint. Late results of closed reduction and arthrographic studies of recent cases. Acta Chir Scand. 1941; 84(Suppl 63):1–142.11. Karakaş ES, Baktir A, Argün M, Türk CY. One-stage treatment of congenital dislocation of the hip in older children. J Pediatr Orthop. 1995; 15:330–336. PMID: 7790490.
Article12. Ning B, Yuan Y, Yao J, Zhang S, Sun J. Analyses of outcomes of one-stage operation for treatment of late-diagnosed developmental dislocation of the hip: 864 hips followed for 3.2 to 8.9 years. BMC Musculoskelet Disord. 2014; 15:401. PMID: 25432778.
Article13. Dogan M, Bozkurt M, Sesen H, Yildirim H. One-stage treatment of congenital severely dislocated hips in older children through various acetabuloplasty techniques: 22 children followed for 1–5 years. Acta Orthop. 2005; 76:212–219. PMID: 16097546.14. Wada A, Fujii T, Takamura K, Yanagida H, Taketa M, Nakamura T. Pemberton osteotomy for developmental dysplasia of the hip in older children. J Pediatr Orthop. 2003; 23:508–513. PMID: 12826952.
Article15. Browne RS. The management of late diagnosed congenital dislocation and subluxation of the hip-with special reference to femoral shortening. J Bone Joint Surg Br. 1979; 61:7–12. PMID: 422637.
Article16. Forlin E, Munhoz da Cunha LA, Figueiredo DC. Treatment of developmental dysplasia of the hip after walking age with open reduction, femoral shortening, and acetabular osteotomy. Orthop Clin North Am. 2006; 37:149–160. viPMID: 16638446.
Article17. Ganger R, Radler C, Petje G, Manner HM, Kriegs-Au G, Grill F. Treatment options for developmental dislocation of the hip after walking age. J Pediatr Orthop B. 2005; 14:139–150. PMID: 15812282.
Article18. Galpin RD, Roach JW, Wenger DR, Herring JA, Birch JG. One-stage treatment of congenital dislocation of the hip in older children, including femoral shortening. J Bone Joint Surg Am. 1989; 71:734–741. PMID: 2732262.
Article19. Vukasinović Z, Spasovski D, Zivković Z, Slavković N, Cerović S. Triple pelvic osteotomy in the treatment of hip dysplasia. Srp Arh Celok Lek. 2009; 137:239–248. PMID: 19594064.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pediatric Hip Disease (I): Diagnosis and Treatment of Developmental Dysplasia of the Hip
- Pediatric Hip Disease (II): Developmental Dysplasia of the Hip – Treatment of Residual Dysplasia
- An Upgrade of the International Hip Dysplasia Institute Classification for Developmental Dysplasia of the Hip
- Dynamic ultrasonography in developmental dysplasia of the hip treated with Pavlik harness
- Augumentation Shelf Operation of Acetabulum for Hip Dysplasia
