Utility of False Profile View for Screening of Ischiofemoral Impingement
- Affiliations
-
- 1Department of Orthopedic Surgery, Yonsei University College of Medicine, Seoul, Korea. wsleeos@yuhs.ac
- 2Department of Radiology, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Rehabilitation, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2427925
- DOI: http://doi.org/10.5371/hp.2018.30.4.219
Abstract
- PURPOSE
Ischiofemoral impingement (IFI)-primarily diagnosed by magnetic resonance imaging (MRI)-is an easily overlooked disease due to its low incidence. The purpose of this study was to evaluate the usefulness of false profile view as a screening test for IFI.
MATERIALS AND METHODS
Fifty-eight patients diagnosed with IFI between June 2013 and July 2017 were enrolled in this retrospective study. A control group (n=58) with matching propensity scores (age, gender, and body mass index) were also included. Ischiofemoral space (IFS) was measured as the shortest distance between the lateral cortex of the ischium and the medial cortex of lesser trochanter in weight bearing hip anteroposterior (AP) view and false profile view. MRI was used to measure IFS and quadratus femoris space (QFS). The receiver operating characteristics (ROC), area under the ROC curve (AUC) and cutoff point of the IFS were measured by false profile images, and the correlation between the IFS and QFS was analyzed using the MRI scans.
RESULTS
In the false profile view and hip AP view, patients with IFI had significantly decreased IFS (P < 0.01). In the false profile view, ROC AUC (0.967) was higher than in the hip AP view (0.841). Cutoff value for differential diagnosis of IFI in the false profile view was 10.3 mm (sensitivity, 88.2%; specificity, 88.4%). IFS correlated with IFS (r=0.744) QFS (0.740) in MRI and IFS (0.621) in hip AP view (P < 0.01).
CONCLUSION
IFS on false profile view can be used as a screening tool for potential IFI.
MeSH Terms
Figure
-
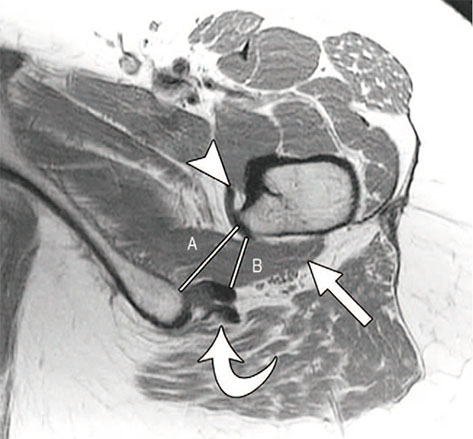
Fig. 1 Diagnosis by magnetic resonance image1). Ischiofemoral space (A) and quadratus femoris space (B) on T2-weighted axial fat-suppressed images on magnetic resonance images as described by Torriani et al6). Iliopsoas tendon (arrowhead), quadratus femoris muscle (straight arrow), and hamstring tendons (curved arrow).
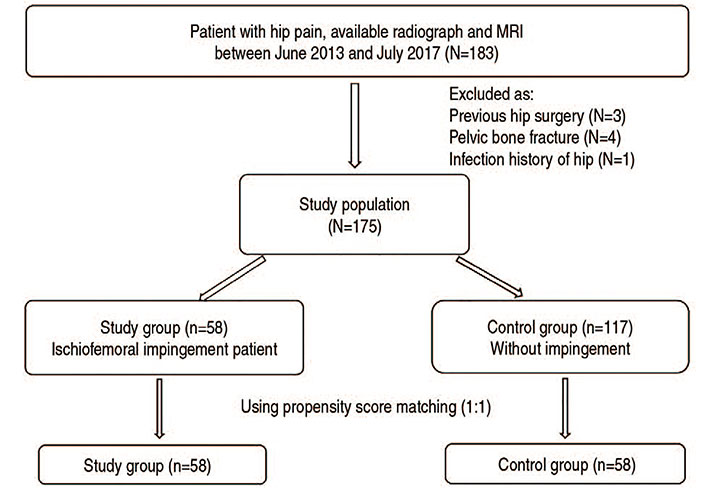
Fig. 2 Flowchart demonstrating patient selection. MRI: magnetic resonance imaging.
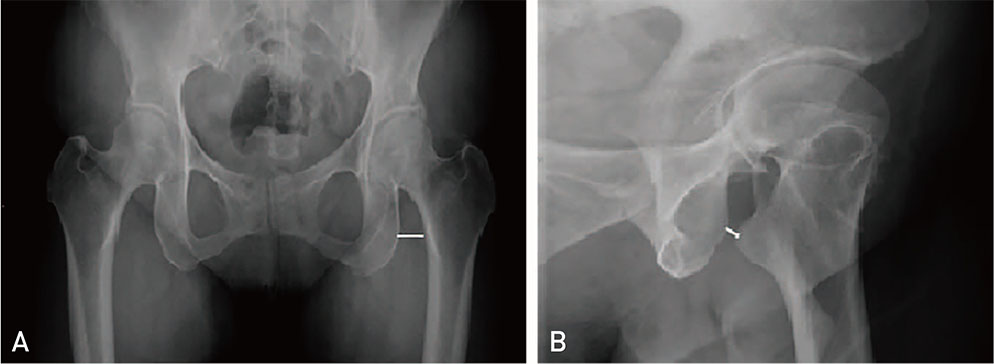
Fig. 3 Ischiofermoal space on the hip standing anteroposterior (A) and false profile view (B) in 68-year-old woman with left hip pain. The shortest distance between the lateral cortex of the ischial tuberosity and the medial cortex of the lesser trochanter.
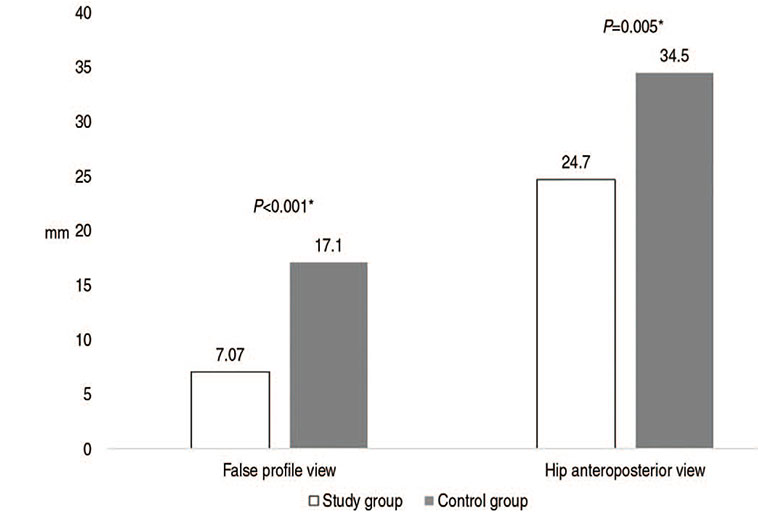
Fig. 4 Comparison of ischiofemoral space value between false profile and hip anteroposterior view.
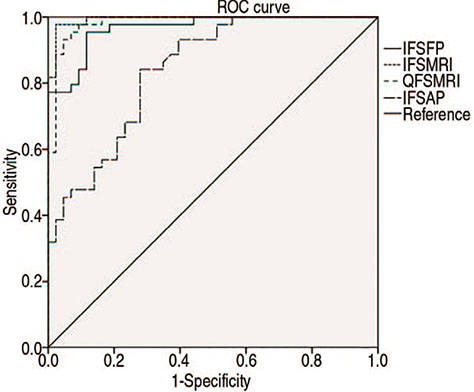
Fig. 5 Receiver operating characteristics (ROC) curve of each parameter. Graph shows ROC curve of each parameter. Ischiofemoral space (IFS) in magnetic resonance imaging (MRI) and quadratus femoris space (QFS) in MRI are almost same and largest area under the ROC curve (AUC). IFS in hip anteroposterior view (IFSAP) exhibits good discriminatory ability, 0.847 (0.80≤AUC<0.90). IFS in false profile view (IFSFP) has much better discriminatory ability, 0.967 (0.90≤AUC).
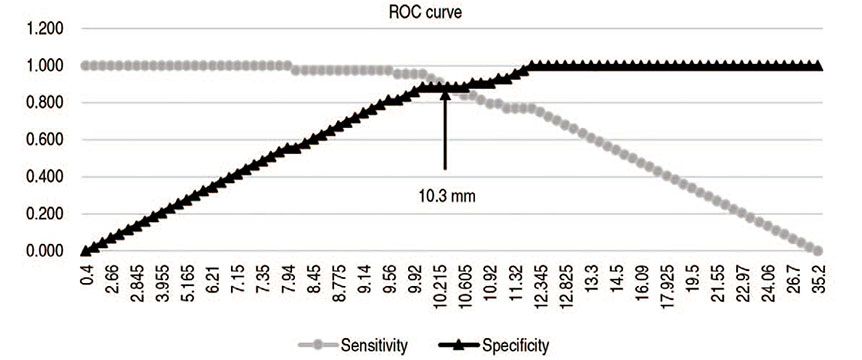
Fig. 6 Cut off value of ischiofemoral space (IFS) in the false profile view. Graph shows sensitivity and specificity values used to discriminate between the study group and the control group. Black curve consisting of triangle shows specificity of IFS in false profile view. Gray curve consisting of circle shows sensitivity of IFS in false profile view. Cut off value was 10.3 mm (sensitivity, 88.6%; specificity, 88.4%). ROC: receiver operating characteristics.
Reference
-
1. Stafford GH, Villar RN. Ischiofemoral impingement. J Bone Joint Surg Br. 2011; 93:1300–1302.
Article2. Patti JW, Ouellette H, Bredella MA, Torriani M. Impingement of lesser trochanter on ischium as a potential cause for hip pain. Skeletal Radiol. 2008; 37:939–941.
Article3. Hernando MF, Cerezal L, Pérez-Carro L, Canga A, González RP. Evaluation and management of ischiofemoral impingement: a pathophysiologic, radiologic, and therapeutic approach to a complex diagnosis. Skeletal Radiol. 2016; 45:771–787.
Article4. Hatem MA, Palmer IJ, Martin HD. Diagnosis and 2-year outcomes of endoscopic treatment for ischiofemoral impingement. Arthroscopy. 2015; 31:239–246.
Article5. Tosun O, Algin O, Yalcin N, Cay N, Ocakoglu G, Karaoglanoglu M. Ischiofemoral impingement: evaluation with new MRI parameters and assessment of their reliability. Skeletal Radiol. 2012; 41:575–587.
Article6. Torriani M, Souto SC, Thomas BJ, Ouellette H, Bredella MA. Ischiofemoral impingement syndrome: an entity with hip pain and abnormalities of the quadratus femoris muscle. AJR Am J Roentgenol. 2009; 193:186–190.
Article7. Clohisy JC, Carlisle JC, Beaulé PE, et al. A systematic approach to the plain radiographic evaluation of the young adult hip. J Bone Joint Surg Am. 2008; 90:Suppl 4. 47–66.
Article8. Bredella MA, Azevedo DC, Oliveira AL, et al. Pelvic morphology in ischiofemoral impingement. Skeletal Radiol. 2015; 44:249–253.
Article9. Schatteman J, Vanhoenacker FM, Somville J, Verstraete KL. Ischiofemoral impingement due to a solitary exostosis. JBR-BTR. 2015; 98:39–42.
Article10. Siebenrock KA, Steppacher SD, Haefeli PC, Schwab JM, Tannast M. Valgus hip with high antetorsion causes pain through posterior extraarticular FAI. Clin Orthop Relat Res. 2013; 471:3774–3780.
Article11. Kwee RM, Ahlawat S, Fritz J. Magnetic resonance imaging findings of ischiofemoral impingement in patients with inflammatory myositis: an observational study. J Comput Assist Tomogr. 2017; 41:212–216.
Article12. Park S, Lee HY, Cuong PM, et al. Supine versus standing radiographs for detecting ischiofemoral impingement: a propensity score-matched analysis. AJR Am J Roentgenol. 2016; 206:1253–1263.
Article13. Lequesne M, de Seze . [False profile of the pelvis. A new radiographic incidence for the study of the hip. Its use in dysplasias and different coxopathies]. Rev Rhum Mal Osteoartic. 1961; 28:643–652.14. Hellman MD, Mascarenhas R, Gupta A, et al. The false-profile view may be used to identify cam morphology. Arthroscopy. 2015; 31:1728–1732.15. Singer AD, Subhawong TK, Jose J, Tresley J, Clifford PD. Ischiofemoral impingement syndrome: a meta-analysis. Skeletal Radiol. 2015; 44:831–837.
Article16. Maras¸ Özdemir Z, Aydlngöz Ü, Görmeli CA, Sağır Kahraman A. Ischiofemoral space on MRI in an asymptomatic population: normative width measurements and soft tissue signal variations. Eur Radiol. 2015; 25:2246–2253.
Article17. Khodair SA, Ghieda UE, Elsayed AS. Ischiofemoral impingement syndrome: spectrum of MRI findings in comparison to normal subjects. Egypt J Radiol Nucl Med. 2014; 45:819–824.
Article18. Papavasiliou A, Siatras T, Bintoudi A, et al. The gymnasts' hip and groin: a magnetic resonance imaging study in asymptomatic elite athletes. Skeletal Radiol. 2014; 43:1071–1077.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ischiofemoral Impingement Syndrome
- Ischiofemoral Impingement Syndrome: Outcomes of Endoscopic Resection of the Lesser Trochanter
- Stress Fracture after Arthroscopic Lesser Trochanter Resection: Diagnosis and Therapy
- A Case of Ischiofemoral Impingement Syndrome as a Differential Diagnosis of Ankylosing Spondylitis
- Study for Acromial Type, Acromial Tilt and Subacromial Distances in Subacromial Impingement Syndrome
