De-novo Gastrointestinal Anastomosis with Lumen Apposing Metal Stent
- Affiliations
-
- 1Division of Gastroenterology and Hepatology, Department of Digestive Diseases and Transplantation, Einstein Healthcare Network, Philadelphia, PA, USA. deepanshu.jain.25@gmail.com
- 2Department of Internal Medicine, Yale-Waterbury Internal Medicine Program, Yale school of medicine, Waterbury, CT, USA.
- 3Department of Internal Medicine, Maulana Azad Medical College, New Delhi, India.
- 4Gastrointestinal Care Consultants PA, Houston, TX, USA.
- KMID: 2427717
- DOI: http://doi.org/10.5946/ce.2018.077
Abstract
- Gastric outlet obstruction, afferent or efferent limb obstruction, and biliary obstruction among patients with altered anatomy often require surgical intervention which is associated with significant morbidity and mortality. Endoscopic dilation for benign etiologies requires multiple sessions, whereas self-expandable metal stents used for malignant etiologies often fail due to tumor in-growth. Lumen apposing metal stents, placed endoscopically with the intent of creating a de-novo gastrointestinal anastomosis bypassing the site of obstruction, can potentially achieve similar efficacy, with a much lower complication rate. In our study cohort (n=79), the composite technical success rate and clinical success rate was 91.1% (72/79) and 97.2% (70/72), respectively. Five different techniques were used: 43% (34/79) underwent the balloon-assisted method, 27.9% (22/79) underwent endoscopic ultrasound-guided balloon occluded gastro-jejunostomy bypass, 20.3% (16/79) underwent the direct technique, 6.3% (5/79) underwent the hybrid rendezvous technique, and 2.5% (2/79) underwent natural orifice transluminal endoscopic surgery (NOTES)-assisted procedure. All techniques required an echoendoscope except NOTES. In all, 53.2% (42/79) had non-cautery enhanced Axios stent, 44.3% (35/79) had hot Axios stent, and 2.5% (2/79) had Niti-S spaxus stent. Symptom-recurrence was seen in 2.8%, and 6.3% had a complication (bleeding, abdominal pain or peritonitis). All procedures were performed by experts at centers of excellence with adequate surgical back up.
MeSH Terms
Figure
-

Fig. 1. Introduction of the guidewire. (A) Endoscopic view of the duodenal stenosis. (B) Fluoroscopic view of the guidewire introduced through the stenosis of the small bowel. (C) Fluoroscopic view of a 20-mm balloon dilator inflated with contrast fluid within the small bowel (Re-produced with permission from Thieme publishers).
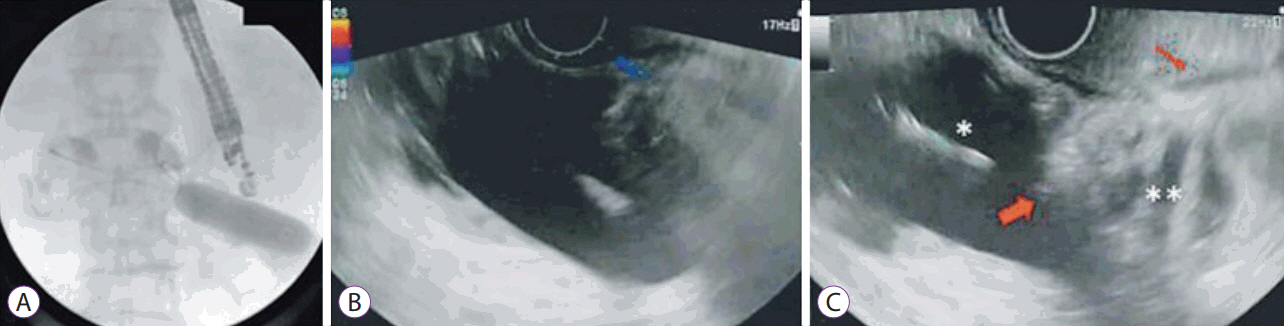
Fig. 2. The balloon dilator inside the small bowel loop. (A) Fluoroscopic view of the echoendoscope in the stomach next to the inflated balloon within the adjacent jejunal loop. (B) Echoendoscopic view showing the inflated balloon. (C) Echoendoscope view showing the inflated balloon (*), the tip of the delivery system of the stent (fat arrow) inside the jejunal lumen (**), and the gastric wall (thin arrow) (Re-produced with permission from Thieme publishers).
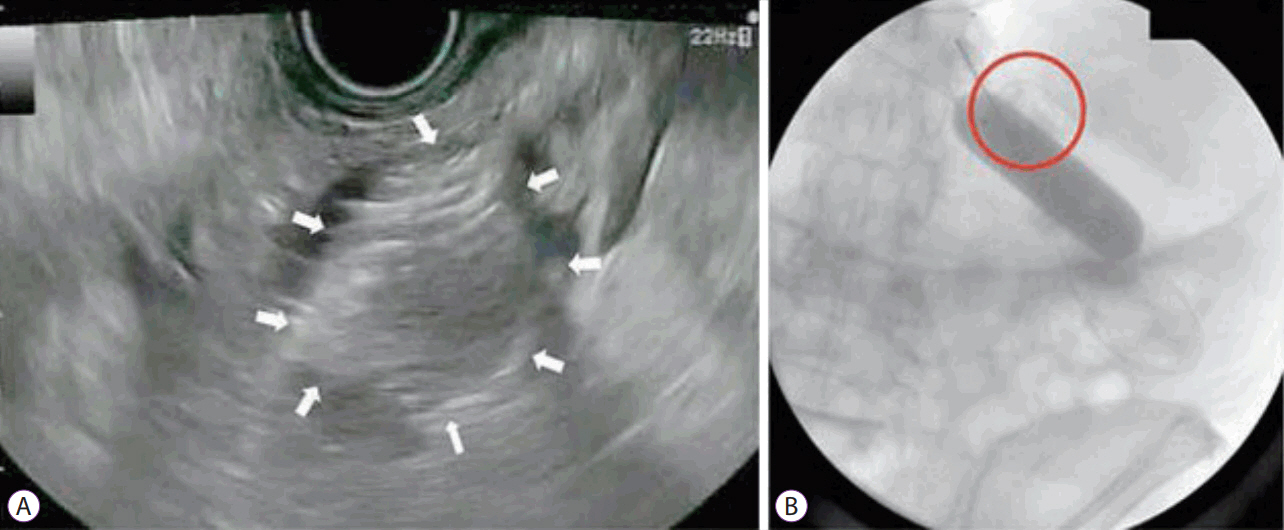
Fig. 3. Deployment of the stent. (A) Echoendoscopic view of the released distal flange of the stent (arrows) into the lumen of the jejunal loop. (B) Fluoroscopic view of the fully released stent (circle) and the intact balloon (Re-produced with permission from Thieme publishers).
Reference
-
1. ASGE Standards of Practice Committee, Fukami N, Anderson MA, et al. The role of endoscopy in gastroduodenal obstruction and gastroparesis. Gastrointest Endosc. 2011; 74:13–21.
Article2. ASGE Standards of Practice Committee, Banerjee S, Cash BD, et al. The role of endoscopy in the management of patients with peptic ulcer disease. Gastrointest Endosc. 2010; 71:663–668.
Article3. Kozarek RA, Botoman VA, Patterson DJ. Long-term follow-up in patients who have undergone balloon dilation for gastric outlet obstruction. Gastrointest Endosc. 1990; 36:558–561.
Article4. Solt J, Bajor J, Szabó M, Horváth OP. Long-term results of balloon catheter dilation for benign gastric outlet stenosis. Endoscopy. 2003; 35:490–495.
Article5. Mittal A, Windsor J, Woodfield J, Casey P, Lane M. Matched study of three methods for palliation of malignant pyloroduodenal obstruction. Br J Surg. 2004; 91:205–209.
Article6. Del Piano M, Ballarè M, Montino F, et al. Endoscopy or surgery for malignant GI outlet obstruction? Gastrointest Endosc. 2005; 61:421–426.
Article7. Khashab M, Alawad AS, Shin EJ, et al. Enteral stenting versus gastrojejunostomy for palliation of malignant gastric outlet obstruction. Surg Endosc. 2013; 27:2068–2075.
Article8. Jain D, Shah M, Patel U, Sharma A, Singhal S. Endoscopic ultrasound guided choledocho-enterostomy by using lumen apposing metal stent in patients with failed endoscopic retrograde cholangiopancreatography: a literature review. Digestion. 2018; 98:1–10.
Article9. Jain D, Bhandari BS, Agrawal N, Singhal S. Endoscopic ultrasound-guided gallbladder drainage using a lumen-apposing metal stent for acute cholecystitis: a systematic review. Clin Endosc. 2018; Jun. 1. [Epub]. https://doi.org.10.5946/ce.2018.024.
Article10. Jain D, Patel U, Ali S, Sharma A, Shah M, Singhal S. Efficacy and safety of lumen-apposing metal stent for benign gastrointestinal stricture. Ann Gastroenterol. 2018; 31:425–438.
Article11. Tyberg A, Perez-Miranda M, Sanchez-Ocaña R, et al. Endoscopic ultrasound-guided gastrojejunostomy with a lumen-apposing metal stent: a multicenter, international experience. Endosc Int Open. 2016; 4:E276–E281.
Article12. Itoi T, Ishii K, Ikeuchi N, et al. Prospective evaluation of endoscopic ultrasonography-guided double-balloon-occluded gastrojejunostomy bypass (EPASS) for malignant gastric outlet obstruction. Gut. 2016; 65:193–195.
Article13. Khashab MA, Kumbhari V, Grimm IS, et al. EUS-guided gastroenterostomy: the first U.S. clinical experience (with video). Gastrointest Endosc. 2015; 82:932–938.
Article14. Khashab MA, Bukhari M, Baron TH, et al. International multicenter comparative trial of endoscopic ultrasonography-guided gastroenterostomy versus surgical gastrojejunostomy for the treatment of malignant gastric outlet obstruction. Endosc Int Open. 2017; 5:E275–E281.
Article15. Chen YI, Kunda R, Storm AC, et al. EUS-guided gastroenterostomy: a multicenter study comparing the direct and balloon-assisted techniques. Gastrointest Endosc. 2018; 87:1215–1221.
Article16. Taunk P, Cosgrove N, Loren DE, Kowalski T, Siddiqui AA. Endoscopic ultrasound-guided gastroenterostomy using a lumen-apposing self-expanding metal stent for decompression of afferent loop obstruction. Endoscopy. 2015; 47 Suppl 1 UCTN:E395–E396.
Article17. Rodrigues-Pinto E, Grimm IS, Baron TH. Efficacy of endoscopically created bypass anastomosis in treatment of afferent limb syndrome: a single-center study. Clin Gastroenterol Hepatol. 2016; 14:633–637.
Article18. Ngamruengphong S, Kumbhari V, Tieu AH, et al. A novel “balloon/snare apparatus” technique to facilitate easy creation of fistula tract during EUS-guided gastroenterostomy. Gastrointest Endosc. 2016; 84:527.19. Perez-Miranda M, Sanchez-Ocaña R, de la Serna Higuera C, Diez-Redondo P, Nuñez H, Vallecillo MA. Transenteric anastomosis with lumen-apposing metal stent as a conduit for iterative endotherapy of malignant biliary obstruction in altered anatomy. Gastrointest Endosc. 2014; 80:339.
Article20. Shah A, Khanna L, Sethi A. Treatment of afferent limb syndrome: novel approach with endoscopic ultrasound-guided creation of a gastrojejunostomy fistula and placement of lumen-apposing stent. Endoscopy. 2015; 47 Suppl 1 UCTN:E309–E310.
Article21. Ikeuchi N, Itoi T, Tsuchiya T, Nagakawa Y, Tsuchida A. One-step EUS-guided gastrojejunostomy with use of lumen-apposing metal stent for afferent loop syndrome treatment. Gastrointest Endosc. 2015; 82:166.
Article22. Majmudar K, Wagh MS. EUS-guided jejuno-jejunostomy with lumen-apposing metal stent for complete jejunal obstruction after gastric bypass. Gastrointest Endosc. 2016; 84:853–854.
Article23. Küllmer A, Wannhoff A, Schmidt A, Caca K. Endoscopic jejunojejunostomy by use of a lumen-apposing self-expandable metal stent for treatment of obstructed efferent loop after subtotal gastrectomy with Roux-en-Y-reconstruction. Video Journal and Encyclopedia of GI Endoscopy. 2017; 2:276–278.
Article24. Tarantino I, Ligresti D, Barresi L, Curcio G, Granata A, Traina M. Onestep, exchange-free, single-balloon-assisted endoscopic ultrasound-guided gastroenterostomy with lumen-apposing metal stent in malignant gastric outlet obstruction. Endoscopy. 2017; 49:E92–E94.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Stent occlusion in endoscopic ultrasound-guided gallbladder drainage from bleeding mitigated by double pigtail plastic stent deployment within lumen apposing metal stent
- Lumen apposing metal stents: A review of current uses and outcomes
- Past, Present, and Future of Gastrointestinal Stents: New Endoscopic Ultrasonography-Guided Metal Stents and Future Developments
- Early Lumen-Apposing Metal Stent Dysfunction Complicating Endoscopic Ultrasound-Guided Gastroenterostomy: A Report of Two Cases
- A remnant choledochal cyst after choledochal cyst excision treated with a lumen-apposing metal stent: a case report
