Analysis of prognostic factors affecting poor outcomes in 41 cases of Fournier gangrene
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Ajou University School of Medicine, Suwon, Korea. i00325@live.co.kr
- KMID: 2426764
- DOI: http://doi.org/10.4174/astr.2018.95.6.324
Abstract
- PURPOSE
We present our experience involving the management of this disease, identifying prognostic factors affecting treatment outcomes.
METHODS
The patients treated for Fournier gangrene at our institution were retrospectively reviewed. Data collected included demographics, extent of soft tissue necrosis, predisposing factors, etiological factors, laboratory values, and treatment outcomes. The severity index and score were calculated. Multivariate regression analysis was used to determine the association between potential predictors and clinical outcomes.
RESULTS
A total of 41 patients (male:female = 33:8) were studied. The mean age was 54.4 years (range, 24-79 years). The most common predisposing factor was diabetes mellitus (n = 19, 46.3%). Sixteen patients (39.0%) were current smokers. Seven patients had chronic kidney disease. The most frequent etiology was urogenital lesion (41.5%). The mortality rate was 22.0% (n = 9). Multivariate regression analyses showed that extension of necrosis beyond perineal/inguinal area and pre-existing chronic kidney disease were significant and independent predictors of mortality. Extension of necrosis beyond perineal/inguinal area was a significant predictor of increased duration in the intensive care unit and hospital stay. In addition, pre-existing chronic kidney disease was a significant predictor of flap reconstruction in the wound.
CONCLUSION
Fournier gangrene with extensive soft tissue necrosis and pre-existing chronic kidney disease was associated with poor prognosis and complexity of patient management. Early recognition of dissemination and premorbid renal function is essential to reduce mortality and establish a management plan for this disease.
MeSH Terms
Figure
-
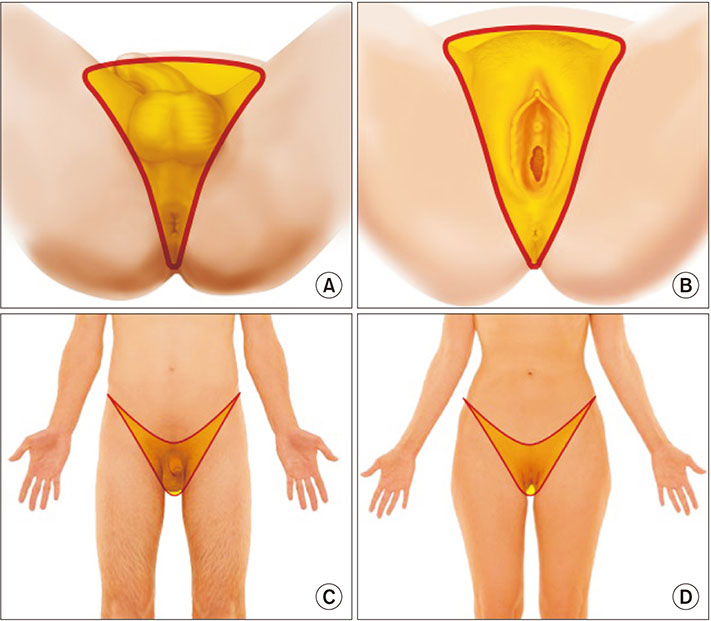
Fig. 1 The anatomic area used for the assessment of dis semination. Inferior (A, B) and frontal views (C, D) in male and female; limited grade refers to gangrene localized in the “Y” area of the perineum, scrotum and penis, vulva, peri anal, or inguinal region. Extended grade disease re fers to extension of the disease beyond these areas.
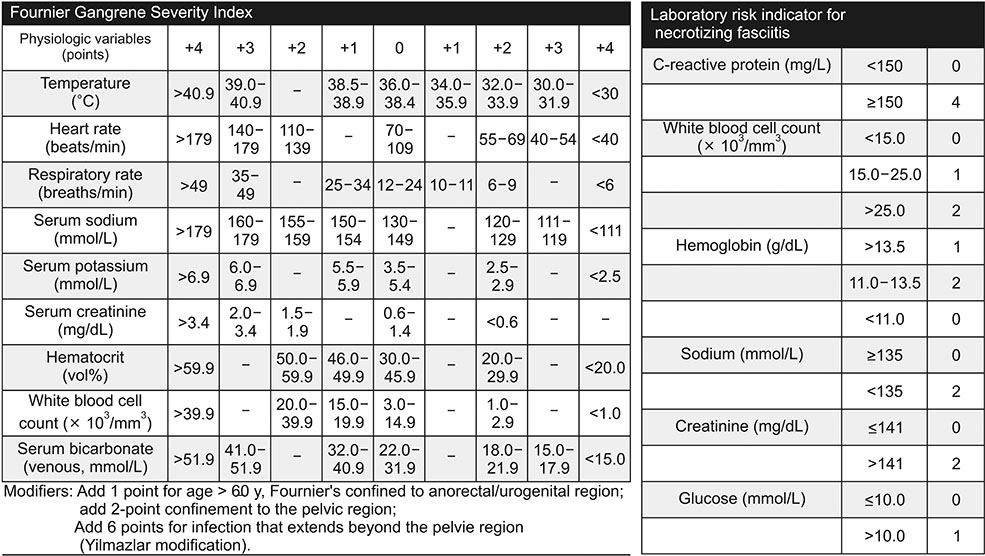
Fig. 2 Fournier Gangrene Severity Index and laboratory risk indicator for necrotizing fasciitis.
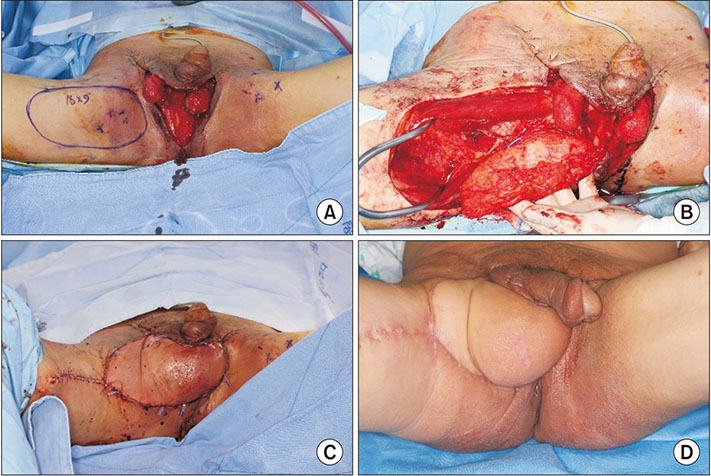
Fig. 3 A case of Fournier gangrene. A 60-year-old male with no past medical history was referred to the Department of Plastic and Reconstructive Surgery for wound reconstruction. Necrotizing fasciitis spread to the perianal area and scrotum, defined as limited grade. (A) After debridement, testicles were exposed. (B) Reconstruction with medial circumflex femoral artery perforator flap. (C) Immediate postoperative view. (D) A photograph obtained 2 weeks postoperatively.
Reference
-
1. Eke N. Fournier's gangrene: a review of 1726 cases. Br J Surg. 2000; 87:718–728.
Article2. Yanar H, Taviloglu K, Ertekin C, Guloglu R, Zorba U, Cabioglu N, et al. Fournier's gangrene: risk factors and strategies for management. World J Surg. 2006; 30:1750–1754.
Article3. Laor E, Palmer LS, Tolia BM, Reid RE, Winter HI. Outcome prediction in patients with Fournier's gangrene. J Urol. 1995; 154:89–92.
Article4. Wong CH, Khin LW, Heng KS, Tan KC, Low CO. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 2004; 32:1535–1541.
Article5. Altarac S, Katusin D, Crnica S, Papes D, Rajkovic Z, Arslani N. Fournier's gangrene: etiology and outcome analysis of 41 patients. Urol Int. 2012; 88:289–293.
Article6. Corcoran AT, Smaldone MC, Gibbons EP, Walsh TJ, Davies BJ. Validation of the Fournier's gangrene severity index in a large contemporary series. J Urol. 2008; 180:944–948.
Article7. Sorensen MD, Krieger JN, Rivara FP, Broghammer JA, Klein MB, Mack CD, et al. Fournier's Gangrene: population based epidemiology and outcomes. J Urol. 2009; 181:2120–2126.
Article8. Garcia Marin A, Martin Gil J, Vaquero Rodriguez A, Sanchez Rodriguez T, de Tomas Palacios J, Lago Oliver J, et al. Fournier's gangrene: analysis of prognostic variables in 34 patients. Eur J Trauma Emerg Surg. 2011; 37:141–145.
Article9. Korkut M, Icoz G, Dayangac M, Akgun E, Yeniay L, Erdogan O, et al. Outcome analysis in patients with Fournier's gangrene: report of 45 cases. Dis Colon Rectum. 2003; 46:649–652.10. Dahm P, Roland FH, Vaslef SN, Moon RE, Price DT, Georgiade GS, et al. Outcome analysis in patients with primary necrotizing fasciitis of the male genitalia. Urology. 2000; 56:31–35.
Article11. Nisbet AA, Thompson IM. Impact of diabetes mellitus on the presentation and outcomes of Fournier's gangrene. Urology. 2002; 60:775–779.
Article12. Ersoz F, Sari S, Arikan S, Altiok M, Bektas H, Adas G, et al. Factors affecting mortality in Fournier's gangrene: experience with fifty-two patients. Singapore Med J. 2012; 53:537–540.13. Jeong HJ, Park SC, Seo IY, Rim JS. Prognostic factors in Fournier gangrene. Int J Urol. 2005; 12:1041–1044.
Article14. Chang FY, Shaio MF. Respiratory burst activity of monocytes from patients with non-insulin-dependent diabetes mellitus. Diabetes Res Clin Pract. 1995; 29:121–127.
Article15. Park SJ, Kim DH, Choi CI, Yun SP, Kim JH, Seo HI, et al. Necrotizing soft tissue infection: analysis of the factors related to mortality in 30 cases of a single institution for 5 years. Ann Surg Treat Res. 2016; 91:45–50.
Article16. Palmer LS, Winter HI, Tolia BM, Reid RE, Laor E. The limited impact of involved surface area and surgical débridement on survival in Fournier's gangrene. Br J Urol. 1995; 76:208–212.17. Benizri E, Fabiani P, Migliori G, Chevallier D, Peyrottes A, Raucoules M, et al. Gangrene of the perineum. Urology. 1996; 47:935–939.
Article18. Yilmazlar T, Ozturk E, Ozguc H, Ercan I, Vuruskan H, Oktay B. Fournier's gangrene: an analysis of 80 patients and a novel scoring system. Tech Coloproctol. 2010; 14:217–223.
Article19. Jones RB, Hirschmann JV, Brown GS, Tremann JA. Fournier's syndrome: necrotizing subcutaneous infection of the male genitalia. J Urol. 1979; 122:279–282.
Article20. Paty R, Smith AD. Gangrene and Fournier's gangrene. Urol Clin North Am. 1992; 19:149–162.
Article
