Two Cases of Corneal Edema Due to Vaporized Amine
- Affiliations
-
- 1Department of Ophthalmology and Visual Science, College of Medicine, The Catholic University of Korea, Seoul, Korea. yangkyeung@hanmail.net
- KMID: 2426370
- DOI: http://doi.org/10.3341/jkos.2018.59.11.1077
Abstract
- PURPOSE
We report two cases of corneal edema in patients who presented with bilateral blurry vision due to vaporized amines while working in a polyurethane processing plant.
CASE SUMMARY
A 28-year-old male presented with bilateral blurred vision. His work involved solidifying polyurethane liquid and he often found himself exposed to polyurethane heat and gas. On examination, the patient's uncorrected visual acuity (UCVA) was 20/40 (right) and 30/50 (left). A slit lamp examination revealed subepithelial microbullae in both eyes. The central corneal thickness (CCT) was also increased in both eyes, measuring 698 µm (right) and 672 µm (left). After prescribing 0.5% moxifloxacin and, 1% fluorometholone eye drops for 3 days in both eyes, the UCVA recovered to 20/40 (right) and 20/20 (left). The CCT decreased to 644 µm (right) and 651 µm (left), and the microbullae improved significantly in the left eye. The second patient was a 34-year-old female who presented with bilateral decreased visual acuity while at work. She worked in a factory that produced car seat filling. Her UCVA was 20/25 (right) and 20/20 (left). The CCT by specular microscopy was 537 µm (right) and 541 µm (left). On slit lamp examination, both eyes demonstrated bilateral central subepithelial edema. The patient did not attend any follow-up outpatient appointments after the initial presentation.
CONCLUSIONS
Exposure to vaporized amines such as polyurethane may causereversible corneal toxicityeven without direct contact. Further consideration should be given to ocular safety and protection from amine compounds in the industrial field.
Keyword
MeSH Terms
Figure
-
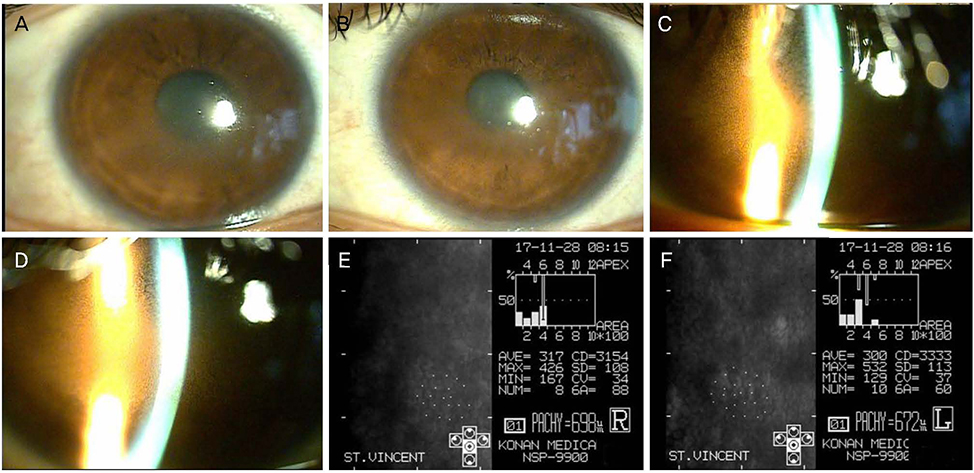
Figure 1 Cornea at first visit of case 1. Edematouscornea by slit lamp microscopic examination (right eye [A], left eye [B]). Subepithelialmicrobulla by slit lamp microscopic examination (right eye [C], left eye [D]). Increased central corneal thickness by specular microscopic examination (right eye [E], left eye [F]) at first visit (case 1). AVE = average cell area; MAX = maximum cell area; MIN = minimum cell area; NUM = number of cell analyzed; CD = cell density; SD = standard deviation of cell area; CV = coefficient of variation; 6A = hexagonality.
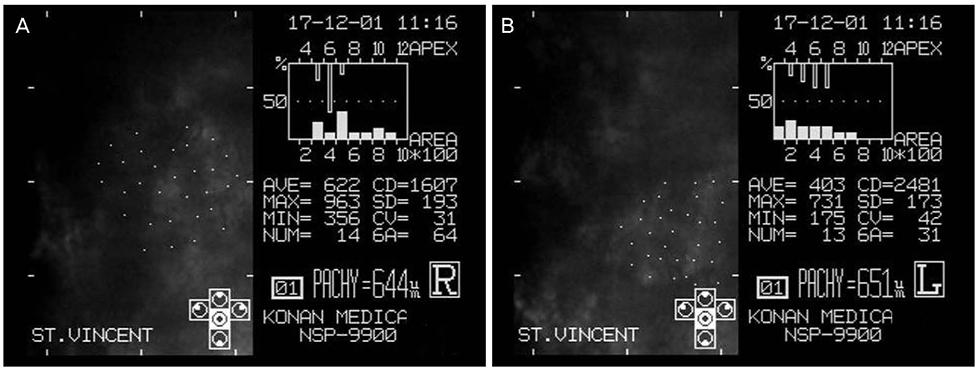
Figure 2 Cornea at second visit of case 1. Decreased cornea edema by specular microscopic examination at second visit (right eye [A], left eye [B]) (case 1). AVE = average cell area; MAX = maximum cell area; MIN = minimum cell area; NUM = number of cell analyzed; CD = cell density; SD = standard deviation of cell area; CV = coefficient of variation; 6A = hexagonality.
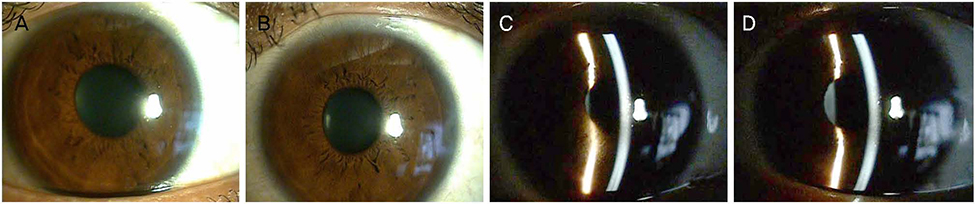
Figure 3 Cornea at third visit of case 1. Slight remained cornea edema by slit lamp microscopic examinationat third visit (right eye [A], left eye [B]). Decreased subepithelial microbulla by slit lamp microscopic examination at third visit (right eye [C], left eye [D]) (case 1).

Figure 4 Cornea at first visit of case 2. Mild central subepithelial edema was observed by slit lamp microscopic examination (right eye [A], left eye [B]) but central corneal thickness by specular microscopic examination was within normal range (right eye [C], left eye [D]) at first visit (case 2). AVE = average cell area; MAX = maximum cell area; MIN = minimum cell area; NUM = number of cell analyzed; CD = cell density; SD = standard deviation of cell area; CV = coefficient of variation; 6A = hexagonality.
Reference
-
1. Bingham E, Cohrssen B. Patty's Toxicology. 6th ed. New York: John Wiley & Sons;2012. Vol. 1:p. 433–516.2. Ballantyne B. Glaucopsia: an occupational ophthalmic hazard. Toxicol Rev. 2004; 23:83–90.3. Järvinen P, Engström K, Riihimäki V, et al. Effects of experimental exposure to triethylamine on vision and the eye. Occup Environ Med. 1999; 56:1–5.4. Michelotti MM, Gupta C, Hood CT. Persistent amine keratopathy secondary to indirect exposure to spray polyurethane foam insulation. JAMA Ophthalmol. 2015; 133:e1584.
Article5. Potts AM, Rouse EF, Eiferman RA, Au PC. An unusual type of keratopathy observed in polyurethane workers and its reproduction in experimental animals. Am J Ind Med. 1986; 9:203–213.
Article6. Page EH, Cook CK, Hater MA, et al. Visual and ocular changes associated with exposure to two tertiary amines. Occup Environ Med. 2003; 60:69–75.
Article7. Jang JK. Amines as occupational hazards for visual disturbance. Ind Health. 2016; 54:101–115.
Article8. Dernehl CU. Health hazards associated with polyurethane foams. J Occup Med. 1966; 8:59–62.9. Mellerio J, Weale RA. Hazy vision in amine plant operatives. Br J Ind Med. 1966; 23:153–154.
Article10. Albrecht WN, Stephenson RL. Health hazards of tertiary amine catalysts. Scand J Work Environ Health. 1988; 14:209–219.
Article11. Goldberg ME, Johnson HE. Autonomic ganglion activity and acute toxicologic effects of N,N,N',N'-tetramethyl-1, 3-butanediamine and triethylenediamine, two foam catalyst amines. Toxicol Appl Pharmacol. 1962; 4:522–545.12. Jang JK, Park H. A case of workers' exposure reductions for chemicals in a polyurethane pad process through the substitution of raw materials. J Korean Soc Occup Environ Hyg. 2014; 24:281–292.
Article13. Beare JD. Eye injuries from assault with chemicals. Br J Ophthalmol. 1990; 74:514–518.
Article14. Kuckelkorn R, Schrage N, Keller G, Redbrake C. Emergency treatment of chemical and thermal eye burns. Acta Ophthalmol Scand. 2002; 80:4–10.
Article15. Sharma N, Kaur M, Agarwal T, et al. Treatment of acute ocular chemical burns. Surv Ophthalmol. 2018; 63:214–235.
Article
