An anomalous portal vein crossing the lesser sac and ending at the upper part of ductus venosus
- Affiliations
-
- 1Department of Surgery and Biomedical Research Institute, Chonbuk National University Hospital, Jeonju, Korea.
- 2Department of Anatomy, Chonbuk National University Medical School, Jeonju, Korea. 407kk@hanmail.net
- 3Division of Internal Medicine, Iwamizawa Asuka Hospital, Iwamizawa, Japan.
- 4Institute of Embryology, Universidad Complutense, Madrid, Spain.
- KMID: 2424826
- DOI: http://doi.org/10.5115/acb.2015.48.3.218
Abstract
- In serial sagittal sections of a fetus on week 9 (crown-rump length, 36 mm), we incidentally found absence of the usual portal vein through the hepatoduodenal ligament. Instead, an anomalous portal vein originated behind the pancreatic body, crossed the lesser sac and merged with the upper part of the ductus venosus. During the course across the lesser sac, the vein provided a deep notch of the liver caudate lobe (Spiegel's lobe). The hepatoduodenal ligament contained the hepatic artery, the common bile duct and, at the right posterior margin of the ligament, and a branch of the anomalous portal vein which communicated with the usual right branch of the portal vein at the hepatic hilum. The umbilical portion of the portal vein took a usual morphology and received the umbilical vein and gave off the ductus venosus. Although it seemed not to be described yet, the present anomalous portal vein was likely to be a persistent left vitelline vein. The hepatoduodenal ligament was unlikely to include the left vitelline vein in contrast to the usual concept.
MeSH Terms
Figure
-
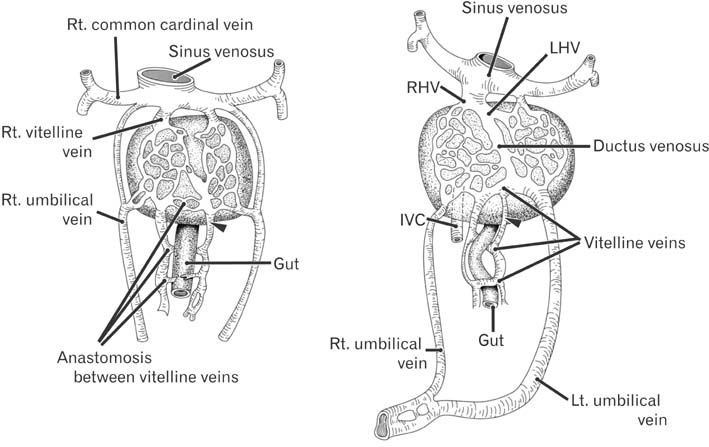
Fig. 1 Usual diagrams showing development of the portal vein. The vitelline veins provide sinusoids in the liver (left-hand side panel) and the extrahepatic portal vein course uses some of communications between the left and right vitelline veins: the final portal vein first crosses the ventral aspect of the gut and, next, it crosses the dorsal aspect of the gut. The left vitelline vein near the liver (arrowhead) is not used for the final portal vein. IVC, inferior vena cava; LHV, left hepatic vein; RHV, right hepatic vein. This figure omits details of the inferior vena cava development shown in our previous study [4].
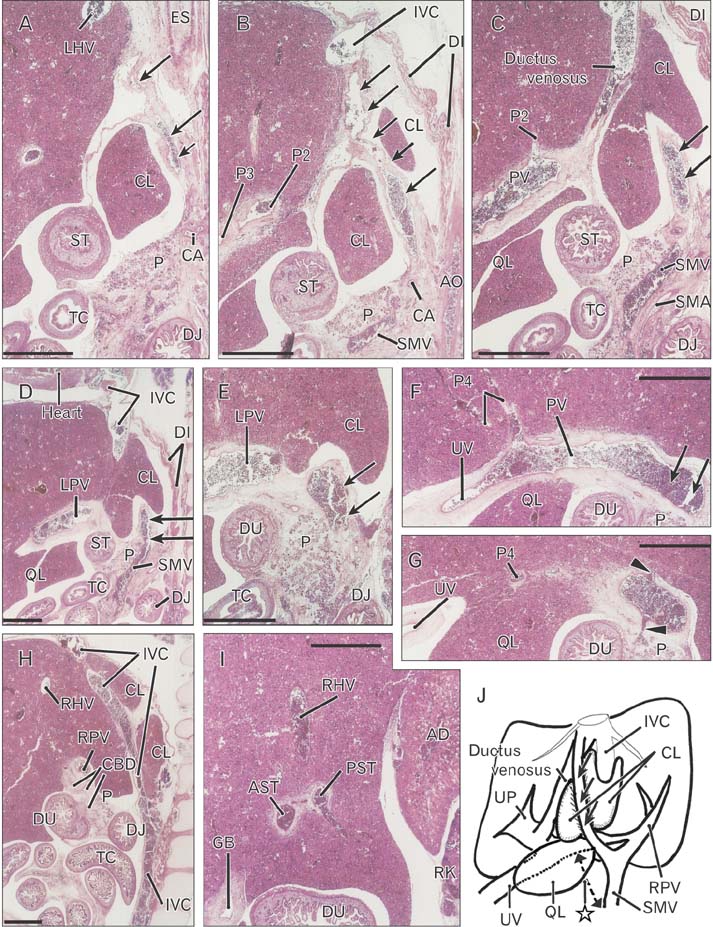
Fig. 2 Anomalous portal vein seen in a 36-mm fetus. Sagittal sections. Hematoxylin and eosin staining. Panel (A) (or panel I) displays the most left (or right) side of the figure. The lesser sac contains liver caudate lobe (CL; panels A-E). An anomalous portal vein (arrows) provides a peritoneal fold crossing the lesser sac. The vein is originated from the superior mesenteric vein (SMV) (D) and ends at the ductus venosus (B). A branch of the anomalous portal vein joins the usual right portal vein (RPV) in panel (F). In panel (F), PV indicates the usual site of the hilar bifurcation of the portal vein. The right portal vein issues branches to the pancreas (P) and segment 6 of the liver (arrowheads in panel G) and it divides into the right anterior and posterior sectorial trunks (AST, PST) of the liver (I). Panel (H) includes the usual longitudinal course of the inferior vena cava (IVC). Panel (J) exhibits a schematic representation of the portal vein configuration: dotted line with star indicates the usual portal vein course. Intervals between panels are 0.2 mm (A-B), 0.3 mm (B-C), 0.2 mm (C-D), 0.3 mm (D-E), 0.2 mm (E-F, F-G), 0.4 mm (G-H), and 0.6 mm (H-I), respectively. Panels (A), (B), (C), (E), (F), and (G) or panels (D) and (H) are prepared at the same magnification. Scale bars=1 mm. AD, right adrenal; AO, aorta; CA, celiac artery; CBD, common bile duct; DI, diaphragm; DJ, duodenojejunal junction; DU, duodenum; ES, esophagus; GB, gall bladder; LHV, left hepatic vein; LPV, left branch of the portal vein; P2, P3, and P4, portal vein branches to segment 2-4, respectively; QL, quadrate lobe of the liver; RHV, right hepatic vein; RK, right kidney; SMA, superior mesenteric artery; ST, stomach; TC, transverse colon; UP, umbilical portion of the portal vein; UV, umbilical vein.

Fig. 3 Understanding of the present anomaly as a left vitelline vein. The usual portal vein course behind the duodenum is closed and, instead, the portal vein used a part of the left vitelline vein course (see also Fig. 1). IMV, inferior mesenteric vein; IVC, inferior vena cava; SMV, superior mesenteric vein; SPV, splenic vein. The closure of the right umbilical vein is normal.
Reference
-
1. Collardeau-Frachon S, Scoazec JY. Vascular development and differentiation during human liver organogenesis. Anat Rec (Hoboken). 2008; 291:614–627.2. Inoue M, Taenaka N, Nishimura S, Kawamura T, Aki T, Yamaki K, Enomoto H, Kosaka K, Yoshikawa K. Prepancreatic postduodenal portal vein: report of a case. Surg Today. 2003; 33:956–959.3. Tomizawa N, Akai H, Akahane M, Ino K, Kiryu S, Ohtomo K. Prepancreatic postduodenal portal vein: a new hypothesis for the development of the portal venous system. Jpn J Radiol. 2010; 28:157–161.4. Jin ZW, Cho BH, Murakami G, Fujimiya M, Kimura W, Yu HC. Fetal development of the retrohepatic inferior vena cava and accessory hepatic veins: Re-evaluation of the Alexander Barry's hypothesis. Clin Anat. 2010; 23:297–303.5. Yi SQ, Tanaka S, Tanaka A, Shimokawa T, Ru F, Nakatani T. An extremely rare inversion of the preduodenal portal vein and common bile duct associated with multiple malformations. Report of an adult cadaver case with a brief review of the literature. Anat Embryol (Berl). 2004; 208:87–96.6. Dighe M, Vaidya S. Case report. Duplication of the portal vein: a rare congenital anomaly. Br J Radiol. 2009; 82:e32–e34.7. Hwang SE, Cho BH, Hirai I, Kim HT, Kim JH, Fujimiya M, Murakami G, Kimura W. Topographical anatomy of Spiegel's lobe and its adjacent organs in mid-term fetuses: its implication on the development of the lesser sac and adult morphology of the upper abdomen. Clin Anat. 2010; 23:712–719.8. Murakami G, Hata F. Human liver caudate lobe and liver segment. Anat Sci Int. 2002; 77:211–224.9. Kanamura T, Murakami G, Ko S, Hirai I, Hata F, Nakajima Y. Evaluating the hilar bifurcation territory in the human liver caudate lobe to obtain critical information for delimiting reliable margins during caudate lobe surgery: anatomic study of livers with and without the external caudate notch. World J Surg. 2003; 27:284–288.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fetal Intra-abdominal Umbilical Vein Varix Complicated with Patent Ductus Venosus and Atrial Septal Defect
- A Case of Non-Immune Hydrops Fetalis due to Umbilical Venous Malformation and Noonan Syndrome
- Multiple absences of the branches of abdominal aorta with congenital absence of the portal vein, unilateral adrenal agenesis and persistent ductus arteriosus in a female cadaver
- Blood flow volume difference (P-SS) between the portal vein and thesum of splenic vein and superior mesenteric vein in portal hypertension
- Computed Tomography Findings of Thrombosis and Aneurysm of the Portal Venous System
