Hip Pelvis.
2017 Dec;29(4):247-252. 10.5371/hp.2017.29.4.247.
Utility of Radiographs, Computed Tomography, and Three Dimensional Computed Tomography Pelvis Reconstruction for Identification of Acetabular Defects in Residency Training
- Affiliations
-
- 1Department of Orthopaedic Surgery, Wake Forest School of Medicine, Winston-Salem, NC, USA. jplate@wakehealth.edu
- 2Department of Orthopaedic Surgery, Duke University, Durham, NC, USA.
- 3Blue Ridge Bone and Joint, Arden, NC, USA.
- KMID: 2424251
- DOI: http://doi.org/10.5371/hp.2017.29.4.247
Abstract
- PURPOSE
The Paprosky classification system of acetabular defects is complex and its reliability has been questioned. The purpose of this study was to evaluate the effectiveness of different radiologic imaging modalities in classifying acetabular defects in revision total hip arthroplasty (THA) and their value of at different levels of training.
MATERIALS AND METHODS
Bone defects in 8 revision THAs were classified by 2 fellowship-trained adult reconstruction surgeons. A timed presentation with representative images for each case (X-ray, two-dimensional computed tomography [CT] and three-dimensional [3D] reconstructions) was shown to 35 residents from the first postgraduate year of training year of training (PGY-1 to PGY-5), 2 adult reconstruction fellows and 2 attending orthopaedic surgeons. The Paprosky classification of bone defects was recorded. The influence of image modality and level of training on classification were analyzed using chi-square analysis (alpha=0.05).
RESULTS
Overall correct classification was 30%. The level of training had no influence on correct classification (P=0.531). Using X-ray led to 37% correctly identified defects, CT scans to 33% and 3D reconstructions to 20% of correct answers (P < 0.001). There was no difference in correct classification based defect type (P < 0.001). Regardless of level of training or imaging, 64% of observers recognized type 1 defects, compared to only 16% correct recognition of type 3B defects.
CONCLUSION
Using plain X-rays led to an increased number of correct classification, while regular CT scan and 3D CT reconstructions did not improve accuracy. The classification system of acetabular defects can be used for treatment decisions; however, advanced imaging may not improve its utilization.
MeSH Terms
Figure
-

Fig. 1 Anterior-posterior (A) and lateral (B) radiograph of a Paprosky type 2A acetabular defect.
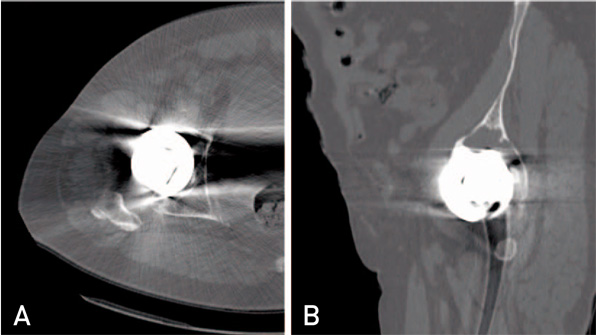
Fig. 2 Selected axial (A) and sagittal (B) computed tomography slices of a Paprosky type 2A acetabular defect.
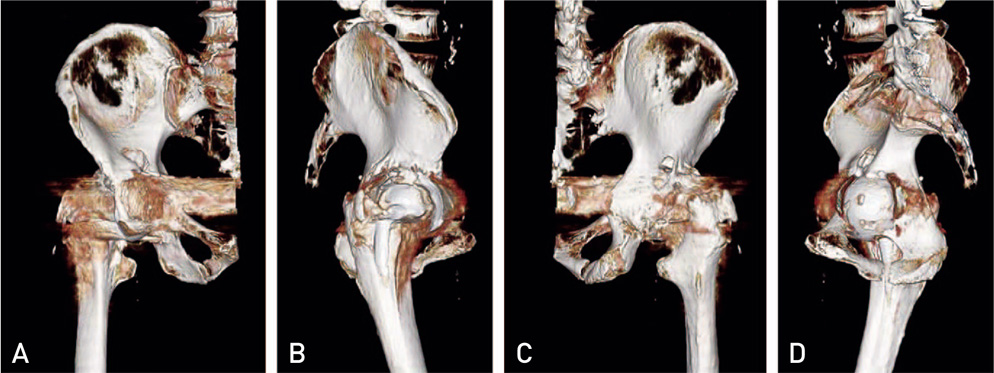
Fig. 3 Screenshots of selected frames (A: anterior, B: lateral, C: posterior, D: medial) from a three-dimensional reconstruction video of a Paprosky type 2A acetabular defect used in the presentation for this study.
Reference
-
1. Paprosky WG, Perona PG, Lawrence JM. Acetabular defect classification and surgical reconstruction in revision arthroplasty. A 6-year follow-up evaluation. J Arthroplasty. 1994; 9:33–44.
Article2. Gozzard C, Blom A, Taylor A, Smith E, Learmonth I. A comparison of the reliability and validity of bone stock loss classification systems used for revision hip surgery. J Arthroplasty. 2003; 18:638–642.
Article3. Parry MC, Whitehouse MR, Mehendale SA, et al. A comparison of the validity and reliability of established bone stock loss classification systems and the proposal of a novel classification system. Hip Int. 2010; 20:50–55.
Article4. Campbell DG, Garbuz DS, Masri BA, Duncan CP. Reliability of acetabular bone defect classification systems in revision total hip arthroplasty. J Arthroplasty. 2001; 16:83–86.
Article5. Munjal S, Leopold SS, Kornreich D, Shott S, Finn HA. CT-generated 3-dimensional models for complex acetabular reconstruction. J Arthroplasty. 2000; 15:644–653.
Article6. Horas K, Arnholdt J, Steinert AF, Hoberg M, Rudert M, Holzapfel BM. Acetabular defect classification in times of 3D imaging and patient-specific treatment protocols. Orthopade. 2017; 46:168–178.
Article7. Garrett J, Halvorson J, Carroll E, Webb LX. Value of 3-D CT in classifying acetabular fractures during orthopedic residency training. Orthopedics. 2012; 35:e615–e620.
Article8. Telleria JJ, Gee AO. Classifications in brief: Paprosky classification of acetabular bone loss. Clin Orthop Relat Res. 2013; 471:3725–3730.
Article9. Hayes AF, Krippendorff K. Answering the call for a standard reliability measure for coding data. Commun Methods Meas. 2007; 1:77–89.
Article10. Yu R, Hofstaetter JG, Sullivan T, Costi K, Howie DW, Solomon LB. Validity and reliability of the Paprosky acetabular defect classification. Clin Orthop Relat Res. 2013; 471:2259–2265.
Article11. Robertson DD, Sutherland CJ, Lopes T, Yuan J. Preoperative description of severe acetabular defects caused by failed total hip replacement. J Comput Assist Tomogr. 1998; 22:444–449.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Usefulness of Three-dimensional Computed Tomography as an Assessment of Periacetabular Osteolysis in Revision Total Hip Arthroplasty
- 3-Dimensional Reconstruction of CT Image
- Assessment of Acetabular Component Anteversion after Total Hip Arthroplasty: Comparison of Anteroposterior and Cross-Table Lateral Radiographs with Computed Tomography Scans
- Three-dimensional imaging modalities in endodontics
- Comprehensive understanding of atrial septal defects by imaging studies for successful transcatheter closure
