Neuromonitoring for Spinal Cord Stimulation Lead Placement Under General Anesthesia
- Affiliations
-
- 1Department of Anesthesiology, Rush University Medical Center, Chicago, IL, USA. Jay_l_shils@rush.edu
- 2Department of Neurosurgery, Beth Israel Deaconess Medical Center, Boston, MA, USA.
- 3Department of Neurosurgery, Harvard Medical School, Boston, MA, USA.
- KMID: 2424171
- DOI: http://doi.org/10.3988/jcn.2018.14.4.444
Abstract
- Spinal cord stimulation (SCS) is a common therapeutic technique for treating medically refractory neuropathic back and other limb pain syndromes. SCS has historically been performed using a sedative anesthetic technique where the patient is awakened at various times during a surgical procedure to evaluate the location of the stimulator lead. This technique has potential complications, and thus other methods that allow the use of a general anesthetic have been developed. There are two primary methods for placing leads under general anesthesia, based on 1) compound muscle action potentials and 2) collisions between somatosensory evoked potentials. Both techniques are discussed, and the literature on SCS lead placement under general anesthesia using intraoperative neurophysiological mapping is comprehensively reviewed.
Keyword
MeSH Terms
Figure
-

Fig. 1 Graphical representation of the activated pathway during the antidromic CMAP technique. The SCS lead stimulates the dorsal column at an intensity that is high enough to activate sufficient large Ia fibers to antidromically excite the alpha motor neurons and generate a CMAP in the muscle. It should be noted that stimulation level is much lower during normal pain therapy, and so no motor activation occurs.8 CMAP: compound muscle action potential, SCS: spinal cord stimulation.
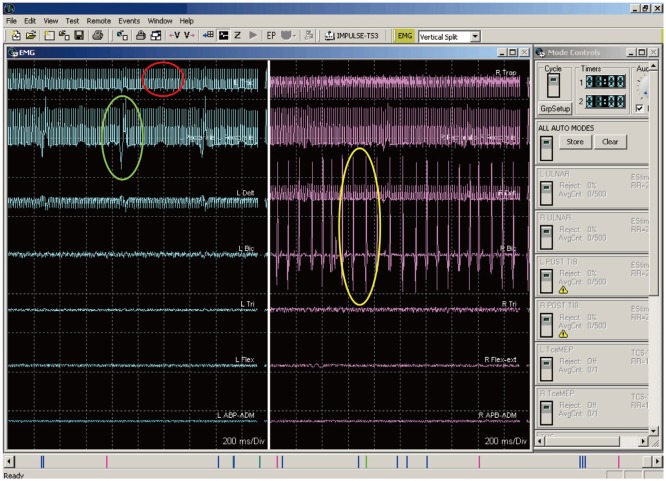
Fig. 2 Three different waveforms, two of which are artifacts. The response in the red circle is an artifact from the stimulation device. The response in the green circle is from an EKG artifact. The responses in the yellow circle are compound muscle action potential generated by the antidromic activation of the alpha motor neuron pool for this muscle group.

Fig. 3 Graphical representation of the stimulation paradigms used for different lead types. The first lead on the left shows the sequence used, with the leftmost electrode pair being the first tested and then sequentially going around the leads testing each electrode pair in a cranial-to-caudal/left-to-right order. A similar pattern is used for the other electrodes.

Fig. 4 Complete activation of all muscles on the right side with no continuous response found on the left side.

Fig. 5 Plot of the location of the spinal cord midline as determined by the technique for each electrode pair. See the text for a detailed description.

Fig. 6 Graphical representation of the basis for the SSEP collision technique. On the left side, the SSEP passes through the sensory pathways uninhibited by any external SCS, thus producing a normal cortical SSEP response. On the right side, the SCS blocks the SSEP stimuli from reaching the cortex, resulting in no cortical SSEP response. See the text for more details. SCS: spinal cord stimulation, SSEP: standard somatosensory evoked potential.

Fig. 7 A collision occurs when the SCS-generated antidromic AP and the SSEP-generated orthodromic AP meet at the same point while they are traveling in opposite directions. When this occurs no AP reaches the cortex to generate a response. In some very rare situations the stimuli may be sufficiently out of phase to allow an SSEP AP to pass undisturbed. However, the large difference between the SCS rate and the SSEP stimulation rate makes this condition highly unlikely. AP: action potentials, SCS: spinal cord stimulation, SSEP: standard somatosensory evoked potential.
Reference
-
1. Zhang K, Bhatia S, Oh M, Whiting D. Epidural anesthesia for placement of spinal cord stimulators with paddle-type electrodes. Stereotact Funct Neurosurg. 2009; 87:292–296. PMID: 19590261.
Article2. Vangeneugden J. Implantation of surgical electrodes for spinal cord stimulation: classical midline laminotomy technique versus minimal invasive unilateral technique combined with spinal anaesthesia. Acta Neurochir Suppl. 2007; 97:111–114.
Article3. Skipsey IG, Colvin JR, Mackenzie N, Kenny GN. Sedation with propofol during surgery under local blockade. Assessment of a target-controlled infusion system. Anaesthesia. 1993; 48:210–213. PMID: 8460797.4. Mingus ML, Monk TG, Gold MI, Jenkins W, Roland C. Remifentanil versus propofol as adjuncts to regional anesthesia. Remifentanil 3010 Study Group. J Clin Anesth. 1998; 10:46–53. PMID: 9526938.5. Holsheimer J, Barolat G, Struijk JJ, He J. Significance of the spinal cord position in spinal cord stimulation. Acta Neurochir Suppl. 1995; 64:119–124. PMID: 8748598.
Article6. Holsheimef J, Barolat G. Spinal geometry and paresthesia coverage in spinal cord stimulation. Neuromodulation. 1998; 1:129–136. PMID: 22150980.
Article7. Bhananker SM, Posner KL, Cheney FW, Caplan RA, Lee LA, Domino KB. Injury and liability associated with monitored anesthesia care: a closed claims analysis. Anesthesiology. 2006; 104:228–234. PMID: 16436839.8. Shils JL, Arle JE. Intraoperative neurophysiologic methods for spinal cord stimulator placement under general anesthesia. Neuromodulation. 2012; 15:560–571. PMID: 22672099.
Article9. Mammis A, Mogilner AY. The use of intraoperative electrophysiology for the placement of spinal cord stimulator paddle leads under general anesthesia. Neurosurgery. 2012; 70:230–236. PMID: 21869720.
Article10. Falowski SM, Celii A, Sestokas AK, Schwartz DM, Matsumoto C, Sharan A. Awake vs. asleep placement of spinal cord stimulators: a cohort analysis of complications associated with placement. Neuromodulation. 2011; 14:130–134. PMID: 21992199.
Article11. Schoen N, Chieng LO, Madhavan K, Jermakowicz WJ, Vanni S. The use of intraoperative electromyogram during spinal cord stimulator placement surgery: a case series. World Neurosurg. 2017; 100:74–84. PMID: 28034811.
Article12. Tamkus AA, Scott AF, Khan FR. Neurophysiological monitoring during spinal cord stimulator placement surgery. Neuromodulation. 2015; 18:460–464. PMID: 25677059.
Article13. Roth SG, Lange S, Haller J, De La Cruz P, Kumar V, Wilock M, et al. A prospective study of the intra- and postoperative efficacy of intraoperative neuromonitoring in spinal cord stimulation. Stereotact Funct Neurosurg. 2015; 93:348–354. PMID: 26444517.
Article14. Air EL, Toczyl GR, Mandybur GT. Electrophysiologic monitoring for placement of laminectomy leads for spinal cord stimulation under general anesthesia. Neuromodulation. 2012; 15:573–579. PMID: 23205816.
Article15. Collison C, Prusik J, Paniccioli S, Briotte M, Grey R, Feustel P, et al. Prospective study of the use of intraoperative neuromonitoring in determining post-operative energy requirements and physiologic midline in spinal cord stimulation. Neuromodulation. 2017; 20:575–581. PMID: 28370852.16. Davidoff RA. Handbook of the Spinal Cord: Anatomy and Physiology (Vols 2 and 3). New York, NY: Dekker Publishing;1984. p. 318.17. Balzer JR, Tomycz ND, Crammond DJ, Habeych M, Thirumala PD, Urgo L, et al. Localization of cervical and cervicomedullary stimulation leads for pain treatment using median nerve somatosensory evoked potential collision testing. J Neurosurg. 2011; 114:200–205. PMID: 20509731.
Article18. Hunter JP, Ashby P. Segmental effects of epidural spinal cord stimulation in humans. J Physiol. 1994; 474:407–419. PMID: 8014902.
Article19. Schirmer CM, Shils JL, Arle JE, Cosgrove GR, Dempsey PK, Tarlov E, et al. Heuristic map of myotomal innervation in humans using direct intraoperative nerve root stimulation. J Neurosurg Spine. 2011; 15:64–70. PMID: 21476796.
Article20. Arle JE, Mei LZ, Carlson KE, Shils JL. Theoretical effect of DBS on axonal fibers of passage: firing rates, entropy, and information content. Stereotact Funct Neurosurg. 2018; 96:1–12. PMID: 29393267.
Article21. Yingling CD, Hosobuchi Y. Use of antidromic evoked potentials in placement of dorsal cord disc electrodes. Appl Neurophysiol. 1986; 49:36–41. PMID: 3490219.
Article22. Deletis V, Bueno De. Interventional neurophysiological mapping during spinal cord procedures. Stereotact Funct Neurosurg. 2001; 77:25–28. PMID: 12378052.
Article23. Falowski SM, Sharan A, McInerney J, Jacobs D, Venkatesan L, Agnesi F. Nonawake vs Awake Placement of Spinal Cord Stimulators: A Prospective, Multicenter Study Comparing Safety and Efficacy. Neurosurgery. 2018; 3. 14. [Epub] available from: . DOI: 10.1093/neuros/nyy062.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spinal anesthesia for implantation of a spinal cord stimulator in a patient with failed back surgery syndrome: A case report
- Epidural anesthesia for permanent spinal cord stimulation with a cylindrical type lead: a case series
- Cervical Spinal Cord Stimulation Using an 8 Electrode Lead in a Patient with Complex Regional Pain Syndrome Type I: A case report
- Spontaneous Lead Breakage in Implanted Spinal Cord Stimulation Systems
- An Analysis of Paresthesia Areas Evoked by Spinal Cord Stimulation in Relation to the Position of Electrode Tip
