Brain Tumor Res Treat.
2018 Oct;6(2):82-85. 10.14791/btrt.2018.6.e10.
Giant Sellar Xanthogranuloma after Surgical Treatment of Symptomatic Rathke's Cleft Cyst
- Affiliations
-
- 1Department of Neurosurgery, Kosin University Gospel Hospital, Busan, Korea. drchr@hanmail.net
- 2Department of Pathology, Kosin University Gospel Hospital, Busan, Korea.
- KMID: 2423979
- DOI: http://doi.org/10.14791/btrt.2018.6.e10
Abstract
- Extremely massive sellar xanthogranuloma (XG) are rare, and the surgical outcome and prognosis are not well known. XG remain unknown whether they are derived from Rathke's cleft cysts (RCCs) or craniopharyngiomas (CPs) following extensive inflammation and metaplasia, to the point that no epithelium is readily identifiable. These lesions usually tend to occur in younger patients (mean 28.3 years), have a smaller diameter, and remain primarily intrasellar region with infrequent calcification. This 36-year-old man presented our hospital with visual deterioration. At the time of visit, there were no neurological problems other than visual field defect and hormonal disorder. He visited our hospital in 2007 due to headache and decreased vision, and underwent transphenoid surgery for pituitary RCC. Since then, he has received treatment at our hospital for postoperative hormonal disorders. Through preoperative imaging study, the author suspected CP and underwent surgery. During the operation, the adhesion of the tumor to the surrounding major neurovascular structures was severe in the naked eyes, but the tumor could be removed more easily than expected. The postoperative histological findings were confirmed as XG. The postoperative course was uneventful. Compared to the previous literature, this case is a case where the size of XG is very large in a sellar region and it can be proved that it originated from the RCC. And regular follow-up is necessary to confirm the prognosis after surgery.
Keyword
MeSH Terms
Figure
-
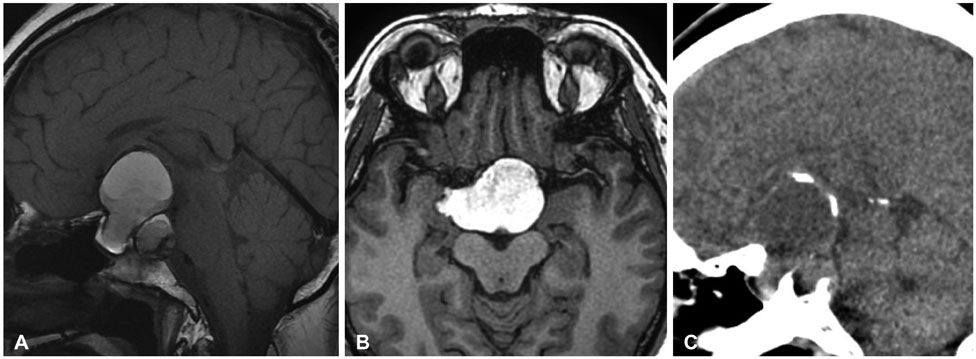
Fig. 1 Preoperative MRI and CT scans. A: T1-weighted imaging reveals heterogeneous intensity of the tumor. B: Sellar tumor extends to the right mesial temporal lobe and prepeduncular cistern on the T1-weighted image. C: Preoperative CT shows calcification in the superior and posterior cystic wall of the tumor.

Fig. 2 Pathological findings. A: Foamy macrophages are found around cholesterol clefts. Inflammatory infiltrates are seen within dense fibrous tissues (hematoxylin and eosin, original magnification ×100). B: Epithelial membranes of the cyst wall are clearly positive for β-catenin (original magnification ×400).

Fig. 3 Postoperative MRI. Tumor is completely removed.
Reference
-
1. Rahmani R, Sukumaran M, Donaldson AM, Akselrod O, Lavi E, Schwartz TH. Parasellar xanthogranulomas. J Neurosurg. 2015; 122:812–817.
Article2. Liu ZH, Tzaan WC, Wu YY, Chen HC. Sellar xanthogranuloma manifesting as obstructive hydrocephalus. J Clin Neurosci. 2008; 15:929–933.
Article3. Kamoshima Y, Sawamura Y, Motegi H, Kubota K, Houkin K. Xanthogranuloma of the sellar region of children: series of five cases and literature review. Neurol Med Chir (Tokyo). 2011; 51:689–693.
Article4. Nishiuchi T, Murao K, Imachi H, et al. Xanthogranuloma of the intrasellar region presenting in pituitary dysfunction: a case report. J Med Case Rep. 2012; 6:119.
Article5. Hernández-Estrada RA, Kshettry VR, Vogel AN, Curtis MT, Evans JJ. Cholesterol granulomas presenting as sellar masses: a similar, but clinically distinct entity from craniopharyngioma and Rathke's cleft cyst. Pituitary. 2017; 20:325–332.
Article6. Yang B, Yang C, Fang J, et al. Clinicoradiologic features and surgical outcomes of sellar xanthogranulomas: a single-center 10-year experience. World Neurosurg. 2017; 99:439–447.
Article7. Dai CX, Guo XS, Liu XH, et al. Xanthogranuloma of the sellar region. Chin Med J (Engl). 2017; 130:249–250.8. Paulus W, Honegger J, Keyvani K, Fahlbusch R. Xanthogranuloma of the sellar region: a clinicopathological entity different from adamantinomatous craniopharyngioma. Acta Neuropathol. 1999; 97:377–382.
Article9. Amano K, Kubo O, Komori T, et al. Clinicopathological features of sellar region xanthogranuloma: correlation with Rathke's cleft cyst. Brain Tumor Pathol. 2013; 30:233–241.
Article10. Miyajima Y, Oka H, Utsuki S, Fujii K. Rathke's cleft cyst with xanthogranulomatous change--case report. Neurol Med Chir (Tokyo). 2011; 51:740–742.11. Hama S, Arita K, Nishisaka T, et al. Changes in the epithelium of Rathke cleft cyst associated with inflammation. J Neurosurg. 2002; 96:209–216.
Article12. Le BH, Towfighi J, Kapadia SB, Lopes MB. Comparative immunohistochemical assessment of craniopharyngioma and related lesions. Endocr Pathol. 2007; 18:23–30.
Article13. Arai A, Nishihara M, Sasayama T, et al. Xanthogranuloma of the sellar region--case report. Neurol Med Chir (Tokyo). 2010; 50:488–491.14. Jung CS, Schänzer A, Hattingen E, Plate KH, Seifert V. Xanthogranuloma of the sellar region. Acta Neurochir (Wien). 2006; 148:473–477.
Article15. Sugata S, Hirano H, Yatsushiro K, Yunoue S, Nakamura K, Arita K. Xanthogranuloma in the suprasellar region. Neurol Med Chir (Tokyo). 2009; 49:124–127.16. Hofmann BM, Kreutzer J, Saeger W, et al. Nuclear beta-catenin accumulation as reliable marker for the differentiation between cystic craniopharyngiomas and rathke cleft cysts: a clinico-pathologic approach. Am J Surg Pathol. 2006; 30:1595–1603.
Article17. Buslei R, Nolde M, Hofmann B, et al. Common mutations of beta-catenin in adamantinomatous craniopharyngiomas but not in other tumours originating from the sellar region. Acta Neuropathol. 2005; 109:589–597.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Symptomatic Rathke's Cleft Cyst in the Interpeduncular Cistern: Case Report
- Rathke's Cleft Cyst: Case Report
- The Endocrinological Characteristics of Rathke's Cleft Cyst: Pathologically Confirmed in Seven Cases
- Large Ossified Rathke's Cleft Cyst: A Case Report and Review of the Literature
- A case of lymphocytic hypophysitis associated with Rathke's cleft cyst
