Korean J Adult Nurs.
2018 Oct;30(5):536-545. 10.7475/kjan.2018.30.5.536.
The Effect of the Revised Clinical Pathway of Cardiac Rehabilitation on Participation Rates in Patients with Myocardial Infarction: A Retrospective Study
- Affiliations
-
- 1Resident, Department of Rehabilitation Medicine, Chungbuk National University Hospital, Cheongju, Korea.
- 2Assistant Professor, Department of Rehabilitation Medicine, Chungbuk National University Hospital · Chungbuk Regional Cardiocerebrovascular Center, Cheongju, Korea. gjlee1225@gmail.com
- 3Educational Nurse, Chungbuk Regional Cardiocerebrovascular Center, Cheongju, Korea.
- 4Professor, Department of Rehabilitation Medicine, Chungbuk National University College of Medicine · Chungbuk Regional Cardiocerebrovascular Center, Cheongju, Korea.
- KMID: 2423844
- DOI: http://doi.org/10.7475/kjan.2018.30.5.536
Abstract
- PURPOSE
The purpose of this retrospective study was to investigate the effect of revised cardiac rehabilitation Clinical Pathways (CPs) on the Cardiac Rehabilitation (CR) participation rate of patients with Myocardial Infarction (MI) undergoing Percutaneous Coronary Intervention (PCI).
METHODS
We reviewed the electronic medical record of patients who were referred for CR after MI from July 2015 to December 2016. In April 2016, the patient groups were divided into 9-month periods: pre- and post-CP revision. We reduced the mean number of hospital visits for CR and the wait times before starting CR and the first Cardio Pulmonary Exercise (CPX) test. We added a home-based CR program and reinforced the CR liaison nurse's role. The changes in the CR wait time, mean number of hospital visits post-discharge, and participation rates at 1 and 3 months were investigated.
RESULTS
Ninety-two patients were recruited from July 2015 to March 2016. Twenty-four (26.1%) participated in CR at 1 month, and 11 (12.0%) were maintained up to 3 months. From April 2016 to December 2016, 107 patients were recruited. Sixty-five (60.7%) participated at 1 month, and 38 (35.5%) were maintained up to 3 months. The mean number of hospital visits was 3.5±0.8 versus 1.9±0.9 in the previous and revised CP groups. The average number of days to the first CPX test after MI was 43.4±17.6 versus 26.3±10.6.
CONCLUSION
Following CP revision, the CR participation rate significantly improved among patients with PCI post-MI. CP revision in terms of inter-physician communication and additional nursing interventions should be considered.
MeSH Terms
Figure
-
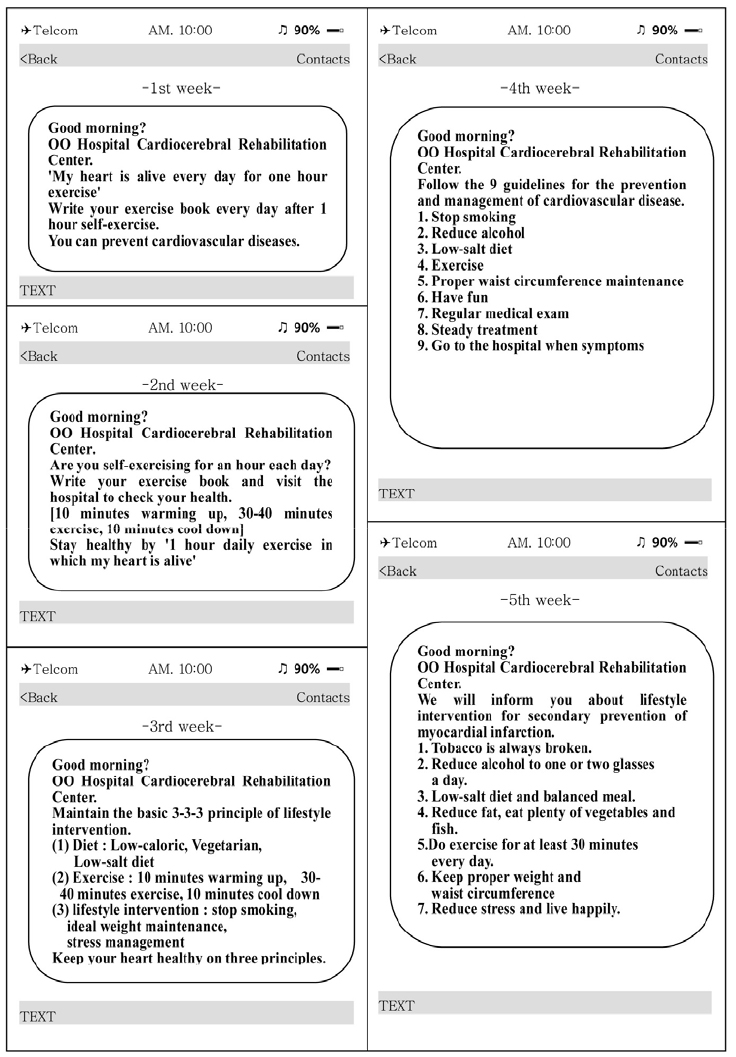
Figure 1 The text messages sent weekly to patients participating in the cardiac rehabilitation.
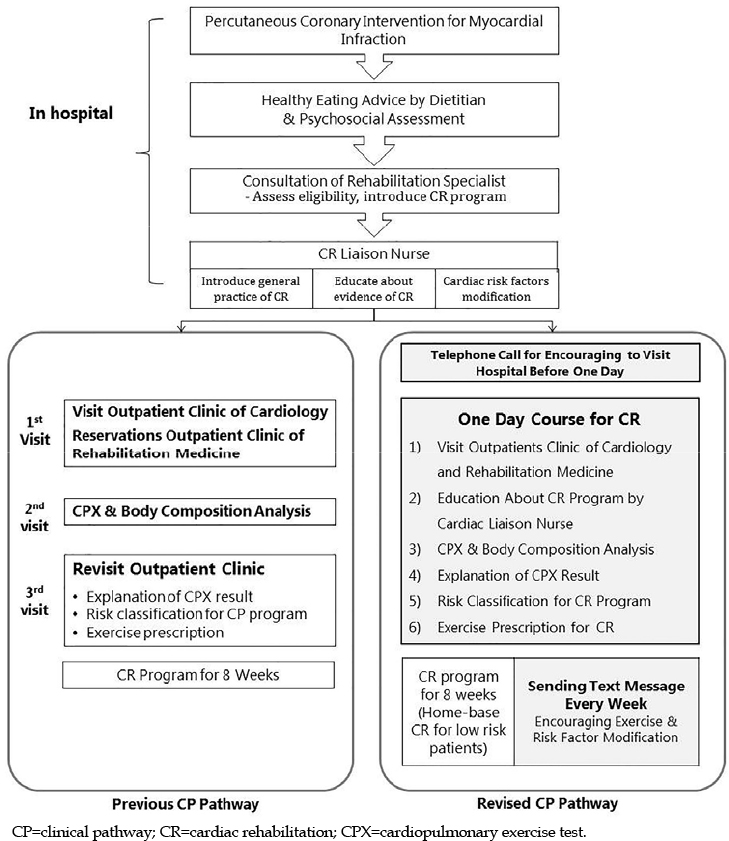
Figure 2 The change in the clinical pathway.
Reference
-
1. Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, et al. Heart disease and stroke statistics--2012 update: a report from the American Heart Association. Circulation. 2012; 125(1):188–197. DOI: 10.1161/cir.0b013e31823ac046.2. Anderson L, Oldridge N, Thompson DR, Zwisler AD, Rees K, Martin N, et al. Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. J Am Coll Cardiol. 2016; 67(1):1–12. DOI: 10.1016/j.jacc.2015.10.044.3. Lawler PR, Filion KB, Eisenberg MJ. Efficacy of exercise-based cardiac rehabilitation post-myocardial infarction: a systematic review and meta-analysis of randomized controlled trials. Am Heart J. 2011; 162(4):571–584.e2. DOI: 10.1016/j.ahj.2011.07.017.
Article4. Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, Bittner VA, et al. Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation. 2013; 128(8):873–934. DOI: 10.1161/cir.0b013e31829b5b44.5. Suaya JA, Shepard DS, Normand SL, Ades PA, Prottas J, Stason WB. Use of cardiac rehabilitation by Medicare beneficiaries after myocardial infarction or coronary bypass surgery. Circulation. 2007; 116(15):1653–1662. DOI: 10.1161/circulationaha.107.701466.
Article6. Grace SL, Angevaare KL, Reid RD, Oh P, Anand S, Gupta M, et al. Effectiveness of inpatient and outpatient strategies in increasing referral and utilization of cardiac rehabilitation: a prospective, multi-site study. Implement Sci. 2012; 7:120. DOI: 10.1186/1748-5908-7-120.
Article7. Dunlay SM, Witt BJ, Allison TG, Hayes SN, Weston SA, Koepsell E, et al. Barriers to participation in cardiac rehabilitation. Am Heart J. 2009; 158(5):852–859. DOI: 10.1016/j.ahj.2009.08.010.
Article8. Daly J, Sindone AP, Thompson DR, Hancock K, Chang E, Davidson P. Barriers to participation in and adherence to cardiac rehabilitation programs: a critical literature review. Prog Cardiovasc Nurs. 2002; 17(1):8–17. DOI: 10.1111/j.0889-7204.2002.00614.x.
Article9. Balady GJ, Ades PA, Bittner VA, Franklin BA, Gordon NF, Thomas RJ, et al. Referral, enrollment, and delivery of cardiac rehabilitation/secondary prevention programs at clinical centers and beyond: a presidential advisory from the American Heart Association. Circulation. 2011; 124(25):2951–2960. DOI: 10.1161/cir.0b013e31823b21e2.10. Stiller JJ, Holt MM. Factors influencing referral of cardiac patients for cardiac rehabilitation. Rehabil Nurs. 2004; 29(1):18–23. DOI: 10.1002/j.2048-7940.2004.tb00295.x.
Article11. Poh R, Ng HN, Loo G, Ooi LS, Yeo TJ, Wong R, et al. Cardiac rehabilitation after percutaneous coronary intervention in a multiethnic Asian country: enrollment and barriers. Arch Phys Med Rehabil. 2015; 96(9):1733–1738. DOI: 10.1016/j.apmr.2015.05.020.
Article12. Grace SL, Scholey P, Suskin N, Arthur HM, Brooks D, Jaglal S, et al. A prospective comparison of cardiac rehabilitation enrollment following automatic vs usual referral. J Rehabil Med. 2007; 39(3):239–245. DOI: 10.2340/16501977-0046.
Article13. Gravely S, Anand SS, Stewart DE, Grace SL. Effect of referral strategies on access to cardiac rehabilitation among women. Eur J Prev Cardiol. 2014; 21(8):1018–1025. DOI: 10.1177/2047487313482280.
Article14. Jolly K, Bradley F, Sharp S, Smith H, Mant D. Follow-up care in general practice of patients with myocardial infarction or angina pectoris: initial results of the SHIP trial. Southampton Heart Integrated Care Project. Fam Pract. 1998; 15(6):548–555. DOI: 10.1093/fampra/15.6.548.
Article15. Russell KL, Holloway TM, Brum M, Caruso V, Chessex C, Grace SL. Cardiac rehabilitation wait times: effect on enrollment. J Cardiopulm Rehabil Prev. 2011; 31(6):373–377. DOI: 10.1097/hcr.0b013e318228a32f.16. Collins ZC, Suskin N, Aggarwal S, Grace SL. Cardiac rehabilitation wait times and relation to patient outcomes. Eur J Phys Rehabil Med. 2015; 51(3):301–309.17. Carlson JJ, Johnson JA, Franklin BA, VanderLaan RL. Program participation, exercise adherence, cardiovascular outcomes, and program cost of traditional versus modified cardiac rehabilitation. Am J Cardiol. 2000; 86(1):17–23. DOI: 10.1016/s0002-9149(00)00822-5.
Article18. Buckingham SA, Taylor RS, Jolly K, Zawada A, Dean SG, Cowie A, et al. Home-based versus centre-based cardiac rehabilitation: abridged Cochrane systematic review and meta-analysis. Open Heart. 2016; 3:e000463. DOI: 10.1136/openhrt-2016-000463.
Article19. American Association of Cardiovascular and Pulmonary Rehabilitation. Guidelines for cardiac rehabilitation and secondary prevention programs. 5th ed. Champaign, IL: Human Kinetics;2013.20. Grace SL, Tan Y, Marcus L, Dafoe W, Simpson C, Suskin N, et al. Perceptions of cardiac rehabilitation patients, specialists and rehabilitation programs regarding cardiac rehabilitation wait times. BMC Health Serv Res. 2012; 12(259):1–9. DOI: 10.1186/1472-6963-12-259.
Article21. Pack QR, Mansour M, Barboza JS, Hibner BA, Mahan MG, Ehrman JK, et al. An early appointment to outpatient cardiac rehabilitation at hospital discharge improves attendance at orientation: a randomized, single-blind, controlled trial. Circulation. 2013; 127(3):349–355. DOI: 10.1161/circulationaha.112.121996.22. Macchi C, Fattirolli F, Lova RM, Conti AA, Luisi MLE, Intini R, et al. Early and late rehabilitation and physical training in elderly patients after cardiac surgery. Am J Phys Med Rehabil. 2007; 86(10):826–834. DOI: 10.1097/phm.0b013e318151fd86.
Article23. Parker K, Stone JA, Arena R, Lundberg D, Aggarwal S, Goodhart D, et al. An early cardiac access clinic significantly improves cardiac rehabilitation participation and completion rates in low-risk ST-elevation myocardial infarction patients. Can J Cardiol. 2011; 27(5):619–627. DOI: 10.1016/j.cjca.2010.12.076.
Article24. JCS Joint Working Group. Guidelines for rehabilitation in patients with cardiovascular disease (JCS 2012). Circ J. 2014; 78(8):2022–2093. DOI: 10.1253/circj.cj-66-0094.25. Clark AM, Haykowsky M, Kryworuchko J, MacClure T, Scott J, DesMeules M, et al. A meta-analysis of randomized control trials of home-based secondary prevention programs for coronary artery disease. Eur J Cardiovasc Prev Rehabil. 2010; 17(3):261–270. DOI: 10.1097/hjr.0b013e32833090ef.
Article26. Blair J, Corrigall H, Angus NJ, Thompson DR, Leslie S. Home versus hospital-based cardiac rehabilitation: a systematic review. Rural Remote Health. 2011; 11(2):1–17.
Article27. Allen JK, Dennison CR. Randomized trials of nursing interventions for secondary prevention in patients with coronary artery disease and heart failure: systematic review. J Cardiovasc Nurs. 2010; 25(3):207–220. DOI: 10.1097/jcn.0b013e3181cc79be.28. Jiang X, Sit JW, Wong TK. A nurse-led cardiac rehabilitation programme improves health behaviours and cardiac physiological risk parameters: evidence from Chengdu, China. J Clin Nurs. 2007; 16(10):1886–1897. DOI: 10.1111/j.1365-2702.2007.01838.x.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cardiac Rehabilitation After Acute Myocardial Infarction Resuscitated From Cardiac Arrest
- The Outcomes of Cardiac Rehabilitation Program in the post Myocardial Infarction patient
- The Impact of Early Regular Cardiac Rehabilitation Program on Myocardial Function after Acute Myocardial Infarction
- The Effects of Cardiac Rehabilitation in Patients with ST Elevation Myocardial Infarction and Non-ST Elevation Myocardial Infarction
- The Effect of Phase 1 Cardiac Rehabilitation Nursing Care on Knowledge, Anxiety and Self-Care Behavior in Patients with Acute Myocardial Infarction
