Trifurcation of right coronary artery and its huge right ventricular branch: can it be hazardous?
- Affiliations
-
- 1Deparment of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal Academy of Higher Education, Manipal, India. nayaksathish@gmail.com
- KMID: 2421179
- DOI: http://doi.org/10.5115/acb.2018.51.2.139
Abstract
- The objective of this case report is to alert the cardiologists and radiologists about the possibility of an extremely rare trifurcation of the right coronary artery. During dissection classes, an early trifurcation of the right coronary artery (RCA) was observed in an adult male cadaver aged approximately 65 years. The RCA had a normal origin from the anterior aortic sinus. After a course of just 2 mm, it trifurcated into a conus artery, a huge right ventricular branch and then a main continuation of the RCA. The conus artery entered the myocardium of the conus after a short course. The huge ventricular branch had a downward and left course almost till the apex of the heart. Right marginal artery was absent. No other vascular variations of heart were observed apart from this. Knowledge of this trifurcation could be useful in coronary angioplasty and bypass procedures.
Keyword
MeSH Terms
Figure
-
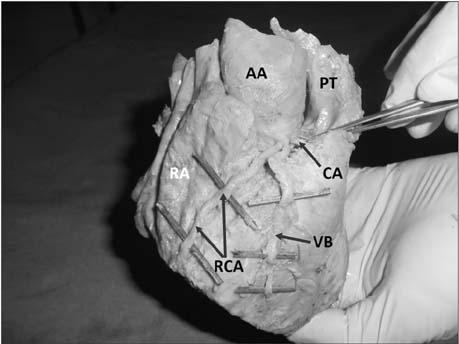
Fig. 1 Dissection of the heart showing the early trifurcation of the right coronary artery. AA, ascending aorta; CA, conus artery; PT, pulmonary trunk; RA, right atrium; RCA, right coronary artery; VB, huge right ventricular branch.

Fig. 2 Superior view of the heart showing single opening of right coronary artery (indicated by the arrow) in the anterior aortic sinus. Ascending aorta has been opened. Pulmonary trunk (PT) can also be seen.
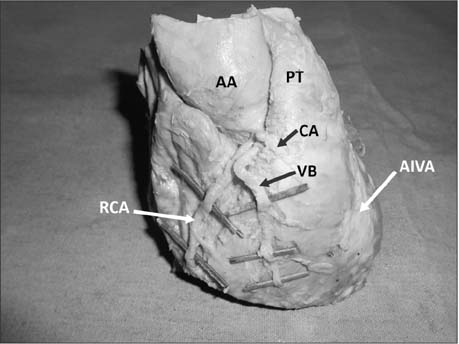
Fig. 3 Front view of the heart showing the right coronary artery and the anterior interventricular artery embedded in the fat. AA, ascending aorta; AIVA, anterior interventricular artery, covered by fat; CA, conus artery; PT, pulmonary trunk; RCA, right coronary artery; VB, huge right ventricular branch.
Cited by 1 articles
-
Novel bilateral bifurcation of the coronary vasculature
Adam Michael Taylor, Joe McAleer, Quenton Wessels
Anat Cell Biol. 2021;54(1):132-135. doi: 10.5115/acb.20.241.
Reference
-
1. Piegger J, Kovacs P, Ambach E. Extremely high origin of the right coronary artery from the ascending aorta. Clin Anat. 2001; 14:369–372.
Article2. Svensson A, Themudo R, Cederlund K. Anomalous origin of right coronary artery from the pulmonary artery. Eur Heart J. 2017; 38:3069.
Article3. Brenner E, Pechriggl E, Zwierzina M, Hörmann R, Moriggl B. Case report: a common trunk of the coronary arteries. Surg Radiol Anat. 2017; 39:455–459.
Article4. Gul M, Sen F, Sahan E, Maden O, Selcuk T. Right coronary artery emerging as a septal branch from the left anterior descending artery: a single coronary ostium anomaly. Herz. 2014; 39:780–782.5. Gholoobi A. Anomalous origin of the right coronary artery from the midportion of the left anterior descending artery: a rare coronary anomaly. J Tehran Heart Cent. 2016; 11:149–152.6. Deora S, Shah S, Patel T. Double or split right coronary artery: still a diagnostic dilemma for this rare coronary anomaly. Int J Cardiol. 2014; 171:457–459.
Article7. Singh S, Ajayi N, Lazarus L, Satyapal KS. Anatomic study of the morphology of the right and left coronary arteries. Folia Morphol (Warsz). 2017; 05. 29. DOI: 10.5603/FM.a2017.0043. [Epub].
Article8. Sánchez-Zuriaga D, Martínez-Soriano F. Absence of circumflex artery with superdominant right coronary: a classic anatomical dissection study. Surg Radiol Anat. 2015; 37:211–214.
Article9. Omeish A. Double-v side-branch stenting followed by main trunk stenting in type-a3 trifurcation coronary artery disease using a dual-catheter technique: the triple-tine fork technique. J Invasive Cardiol. 2013; 25:E198–E202.10. Shao C, Stella PR, Agostoni P. Complex made easy: left anterior descending artery trifurcation lesion completely treated with a single device. J Invasive Cardiol. 2012; 24:E164–E166.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Left Coronary Artery in Korean
- Right Coronary Artery in Korean
- 2 Case of Coronary Artery-to-Left Ventricular Fistulae
- An Unusual Form of Coronary Artery Fistula: A Small Aneurysm of Vieussens' Arterial Ring Communicating with the Pulmonary Artery
- A Case of Open Heart Surgery in a Patient with Huge Sinoatrial Nodal Artery Aneurysm -A case report-
