J Gastric Cancer.
2018 Sep;18(3):209-217. 10.5230/jgc.2018.18.e28.
Surgical Treatment of Gastroesophageal Junction Cancer
- Affiliations
-
- 1Department of Gastroenterological Surgery, Osaka University Graduate School of Medicine, Osaka, Japan. ykurokawa@gesurg.med.osaka-u.ac.jp
- KMID: 2420781
- DOI: http://doi.org/10.5230/jgc.2018.18.e28
Abstract
- Although the incidence of gastroesophageal junction (GEJ) adenocarcinoma has been increasing worldwide, no standardized surgical strategy for its treatment has been established. This study aimed to provide an update on the surgical treatment of GEJ adenocarcinoma by reviewing previous reports and propose recommended surgical approaches. The Siewert classification is widely used for determining which surgical procedure is used, because previous studies have shown that the pattern of lymph node (LN) metastasis depends on tumor location. In terms of surgical approaches for GEJ adenocarcinoma, a consensus was reached based on two randomized controlled trials. Siewert types I and III are treated as esophageal cancer and gastric cancer, respectively. Although no consensus has been reached regarding the treatment of Siewert type II, several retrospective studies suggested that the optimal treatment strategy includes paraaortic LN dissection. Against this background, a Japanese nationwide prospective trial is being conducted to determine the proportion of LN metastasis in GEJ cancers and to identify the optimal extent of LN dissection in each type.
Keyword
MeSH Terms
Figure
-
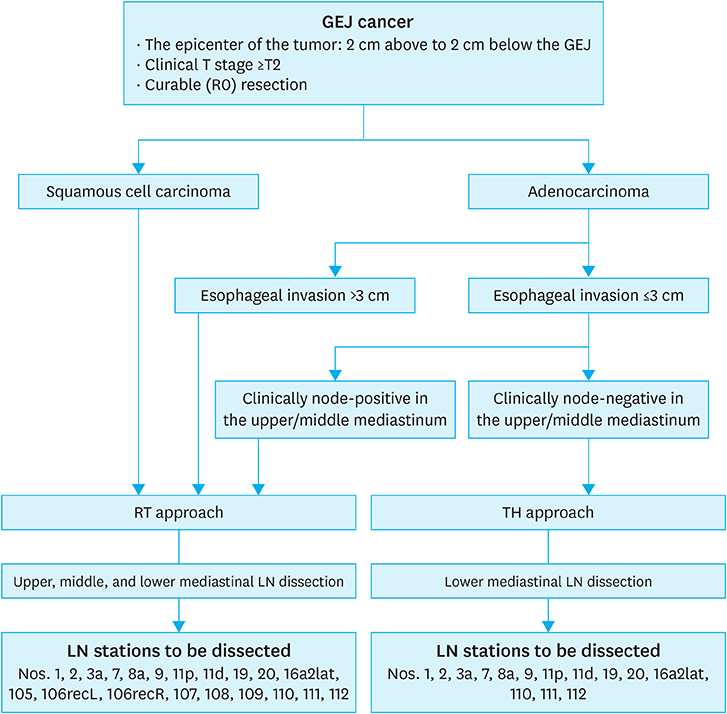
Fig. 1 Schema of the Japanese nationwide prospective trial for GEJ cancer. GFJ = gastroesophageal junction; RT = right transthoracic; TH = transhiatal; LN = lymph node; Nos. = numbers.
Reference
-
1. Blot WJ, Devesa SS, Kneller RW, Fraumeni JF Jr. Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA. 1991; 265:1287–1289.
Article2. Corley DA, Buffler PA. Oesophageal and gastric cardia adenocarcinomas: analysis of regional variation using the cancer incidence in five continents database. Int J Epidemiol. 2001; 30:1415–1425.
Article3. Holmes RS, Vaughan TL. Epidemiology and pathogenesis of esophageal cancer. Semin Radiat Oncol. 2007; 17:2–9.
Article4. Mariette C, Piessen G, Triboulet JP. Therapeutic strategies in oesophageal carcinoma: role of surgery and other modalities. Lancet Oncol. 2007; 8:545–553.
Article5. DeMeester SR. Adenocarcinoma of the esophagus and cardia: a review of the disease and its treatment. Ann Surg Oncol. 2006; 13:12–30.
Article6. Lagergren J, Bergström R, Lindgren A, Nyrén O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999; 340:825–831.
Article7. Kauppila JH, Lagergren J. The surgical management of esophago-gastric junctional cancer. Surg Oncol. 2016; 25:394–400.
Article8. Brierley JD, Gospodarowicz MK, Wittekind C, editors. TNM Classification of Malignant Tumours. 8th ed. Hoboken (NJ): Wiley-Blackwell;2017.9. Siewert JR, Stein HJ. Classification of adenocarcinoma of the oesophagogastric junction. Br J Surg. 1998; 85:1457–1459.
Article10. Misumi A, Murakami A, Harada K, Baba K, Akagi M. Definition of carcinoma of the gastric cardia. Langenbecks Arch Chir. 1989; 374:221–226.
Article11. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011; 14:101–112.12. Japan Esophageal Society. Japanese Classification of Esophageal Cancer. 2nd ed. Tokyo: Japan Esophageal Society;2008.13. Grotenhuis BA, Wijnhoven BP, van Marion R, van Dekken H, Hop WC, Tilanus HW, et al. The sentinel node concept in adenocarcinomas of the distal esophagus and gastroesophageal junction. J Thorac Cardiovasc Surg. 2009; 138:608–612.
Article14. Rüdiger Siewert J, Feith M, Werner M, Stein HJ. Adenocarcinoma of the esophagogastric junction: results of surgical therapy based on anatomical/topographic classification in 1,002 consecutive patients. Ann Surg. 2000; 232:353–361.15. Kurokawa Y, Hiki N, Yoshikawa T, Kishi K, Ito Y, Ohi M, et al. Mediastinal lymph node metastasis and recurrence in adenocarcinoma of the esophagogastric junction. Surgery. 2015; 157:551–555.
Article16. Yoshikawa T, Takeuchi H, Hasegawa S, Nozaki I, Kishi K, Ito S, et al. Theoretical therapeutic impact of lymph node dissection on adenocarcinoma and squamous cell carcinoma of the esophagogastric junction. Gastric Cancer. 2016; 19:143–149.
Article17. Yamashita H, Seto Y, Sano T, Makuuchi H, Ando N, Sasako M, et al. Results of a nation-wide retrospective study of lymphadenectomy for esophagogastric junction carcinoma. Gastric Cancer. 2017; 20:Suppl 1. 69–83.
Article18. Nunobe S, Ohyama S, Sonoo H, Hiki N, Fukunaga T, Seto Y, et al. Benefit of mediastinal and para-aortic lymph-node dissection for advanced gastric cancer with esophageal invasion. J Surg Oncol. 2008; 97:392–395.
Article19. Matsumoto S, Takayama T, Wakatsuki K, Enomoto K, Tanaka T, Migita K, et al. Surgical outcomes for cancer at the gastroesophageal junction. Am Surg. 2012; 78:1285–1291.
Article20. Hulscher JB, van Sandick JW, de Boer AG, Wijnhoven BP, Tijssen JG, Fockens P, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med. 2002; 347:1662–1669.
Article21. Omloo JM, Lagarde SM, Hulscher JB, Reitsma JB, Fockens P, van Dekken H, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the mid/distal esophagus: five-year survival of a randomized clinical trial. Ann Surg. 2007; 246:992–1000.22. Sasako M, Sano T, Yamamoto S, Sairenji M, Arai K, Kinoshita T, et al. Left thoracoabdominal approach versus abdominal-transhiatal approach for gastric cancer of the cardia or subcardia: a randomised controlled trial. Lancet Oncol. 2006; 7:644–651.
Article23. Kurokawa Y, Sasako M, Sano T, Shibata T, Ito S, Nashimoto A, et al. Functional outcomes after extended surgery for gastric cancer. Br J Surg. 2011; 98:239–245.24. Kurokawa Y, Sasako M, Sano T, Yoshikawa T, Iwasaki Y, Nashimoto A, et al. Ten-year follow-up results of a randomized clinical trial comparing left thoracoabdominal and abdominal transhiatal approaches to total gastrectomy for adenocarcinoma of the oesophagogastric junction or gastric cardia. Br J Surg. 2015; 102:341–348.25. Sasako M, McCulloch P, Kinoshita T, Maruyama K. New method to evaluate the therapeutic value of lymph node dissection for gastric cancer. Br J Surg. 1995; 82:346–351.
Article26. Yamashita H, Katai H, Morita S, Saka M, Taniguchi H, Fukagawa T. Optimal extent of lymph node dissection for Siewert type II esophagogastric junction carcinoma. Ann Surg. 2011; 254:274–280.
Article27. Fujitani K, Miyashiro I, Mikata S, Tamura S, Imamura H, Hara J, et al. Pattern of abdominal nodal spread and optimal abdominal lymphadenectomy for advanced Siewert type II adenocarcinoma of the cardia: results of a multicenter study. Gastric Cancer. 2013; 16:301–308.
Article28. Yabusaki H, Nashimoto A, Matsuki A, Aizawa M. Comparison of the surgical treatment strategies for Siewert type II squamous cell carcinoma in the same area as esophagogastric junction carcinoma: data from a single Japanese high-volume cancer center. Surg Today. 2014; 44:1522–1528.
Article29. Mine S, Kurokawa Y, Takeuchi H, Kishi K, Ito Y, Ohi M, et al. Distribution of involved abdominal lymph nodes is correlated with the distance from the esophagogastric junction to the distal end of the tumor in Siewert type II tumors. Eur J Surg Oncol. 2015; 41:1348–1353.
Article30. Hosokawa Y, Kinoshita T, Konishi M, Takahashi S, Gotohda N, Kato Y, et al. Clinicopathological features and prognostic factors of adenocarcinoma of the esophagogastric junction according to Siewert classification: experiences at a single institution in Japan. Ann Surg Oncol. 2012; 19:677–683.
Article31. Pedrazzani C, de Manzoni G, Marrelli D, Giacopuzzi S, Corso G, Minicozzi AM, et al. Lymph node involvement in advanced gastroesophageal junction adenocarcinoma. J Thorac Cardiovasc Surg. 2007; 134:378–385.
Article32. Cense HA, Sloof GW, Klaase JM, Bergman JJ, van Hemert FJ, Fockens P, et al. Lymphatic drainage routes of the gastric cardia visualized by lymphoscintigraphy. J Nucl Med. 2004; 45:247–252.33. de Manzoni G, Pedrazzani C, Di Leo A, Bonfiglio M, Tasselli S, Guglielmi A, et al. Metastases to the para-aortic lymph nodes in adenocarcinoma of the cardia. Eur J Surg. 2001; 167:413–418.34. Hasegawa S, Yoshikawa T, Rino Y, Oshima T, Aoyama T, Hayashi T, et al. Priority of lymph node dissection for Siewert type II/III adenocarcinoma of the esophagogastric junction. Ann Surg Oncol. 2013; 20:4252–4259.
Article35. Mine S, Sano T, Hiki N, Yamada K, Nunobe S, Yamaguchi T. Lymphadenectomy around the left renal vein in Siewert type II adenocarcinoma of the oesophagogastric junction. Br J Surg. 2013; 100:261–266.
Article36. Sasako M, Sano T, Yamamoto S, Kurokawa Y, Nashimoto A, Kurita A, et al. D2 lymphadenectomy alone or with para-aortic nodal dissection for gastric cancer. N Engl J Med. 2008; 359:453–462.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Laparoscopic Gastric Wedge Resection and Prophylactic Antireflux Surgery for a Submucosal Tumor of Gastroesophageal Junction
- Relevance of Position and Movement of the Gastroesophageal Junction in Gastroesophageal Reflux Disease
- Mediastinal Lymph Node Dissection in Gastroesophageal Junction Adenocarcinoma
- A Case of Removal of Coins from Gastroesophageal Junction with Gastroendoscope and Biopsy Forceps
- Relevance of Position and Movement of the Gastroesophageal Junction in Gastroesophageal Reflux Disease: Author's Reply
