Korean Circ J.
2018 Oct;48(10):920-929. 10.4070/kcj.2018.0047.
Fibrosis Marker Soluble ST2 Predicts Atrial Fibrillation Recurrence after Cryoballoon Catheter Ablation of Nonvalvular Paroxysmal Atrial Fibrillation
- Affiliations
-
- 1Department of Cardiology, University of Health Sciences, Adana Health Practices and Research Center, Adana, Turkey.
- 2Department of Cardiology, Mustafa Kemal University, Faculty of Medicine, Hatay, Turkey. onurkaypakli@hotmail.com
- KMID: 2420644
- DOI: http://doi.org/10.4070/kcj.2018.0047
Abstract
- BACKGROUND AND OBJECTIVES
We aimed to investigate the relationship between the recurrence of atrial fibrillation (AF) and fibrosis marker soluble ST2 (sST2) in patients with nonvalvular paroxysmal AF (PAF).
METHODS
We prospectively included 100 consecutive patients with PAF diagnosis and scheduled for cryoballoon catheter ablation for AF (47 males, 53 females; mean age 55.1±10.8 years). sST2 plasma levels were determined using the ASPECT-PLUS assay on ASPECT Reader device (Critical Diagnostics). The measurement range of these measurements was 12.5-250 ng/mL. Patients had regular follow-up visits with 12-lead electrocardiogram (ECG), medical history, and clinical evaluation. Twenty-four hours Holter ECG monitoring had been recorded 12 months after ablation.
RESULTS
AF recurrence was detected in 22 patients after 1 year. Age, smoking history, diabetes mellitus,hypertension frequency, angiotensin converting enzyme inhibitor-angiotensin receptor blocker use, CHA2DS2VASc and HAS-BLED scores, serum sST2 level, left atrium (LA) end-diastolic diameter, LA volume and LA volume index were related to AF recurrence. In multivariable logistic regression analysis, sST2 was found to be only independent parameter for predicting AF recurrence (odds ratio, 1.085; p=0.001). Every 10-unit increase in sST2 was found to be associated with 2.103-fold increase in the risk of AF recurrence. The cut-off value of sST2 obtained by receiver operating characteristic curve analysis was 30.6 ng/mL for prediction of AF recurrence (sensitivity: 77.3%, specificity: 79.5%). The area under the curve was 0.831 (p < 0.001).
CONCLUSIONS
sST2, which is associated with atrial fibrosis, can be thought to be a useful marker for detection of patients with high-grade fibrosis who will get less benefit from cryoablation.
Keyword
MeSH Terms
Figure
-
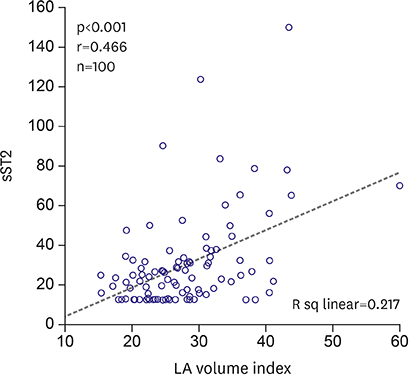
Figure 1 Scatter plot diagram of the relationship of LA volume index with sST2. LA = left atrium; sST2 = soluble ST2.

Figure 2 ROC curve analysis to determine predictive value of sST2 for AF recurrence. AF = atrial fibrillation; AUC = area under the curve; CI = confidence interval; ROC = receiver operating characteristic; sST2 = soluble ST2.
Cited by 1 articles
-
Soluble ST2 in Paroxysmal Atrial Fibrillation: a New Biomarker that Predicts Recurrence?
Ahmed AlTurki
Korean Circ J. 2018;48(10):930-932. doi: 10.4070/kcj.2018.0183.
Reference
-
1. Chugh SS, Havmoeller R, Narayanan K, et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014; 129:837–847.2. Allessie MA, de Groot NM, Houben RP, Schotten U, Boersma E, Smeets JL. Electropathological substrate of long-standing persistent atrial fibrillation in patients with structural heart disease: longitudinal dissociation. Circ Arrhythm Electrophysiol. 2010; 3:606–615.3. Anné W, Willems R, Roskams T, et al. Matrix metalloproteinases and atrial remodeling in patients with mitral valve disease and atrial fibrillation. Cardiovasc Res. 2005; 67:655–666.4. Shinagawa K, Shi YF, Tardif JC, Leung TK, Nattel S. Dynamic nature of atrial fibrillation substrate during development and reversal of heart failure in dogs. Circulation. 2002; 105:2672–2678.
Article5. Sonmez O, Ertem FU, Vatankulu MA, et al. Novel fibro-inflammation markers in assessing left atrial remodeling in nonvalvular atrial fibrillation. Med Sci Monit. 2014; 20:463–470.
Article6. Parikh RH, Seliger SL, Christenson R, Gottdiener JS, Psaty BM, deFilippi CR. Soluble ST2 for prediction of heart failure and cardiovascular death in an elderly, community-dwelling population. J Am Heart Assoc. 2016; 5:e003188.
Article7. Ky B, French B, McCloskey K, et al. High-sensitivity ST2 for prediction of adverse outcomes in chronic heart failure. Circ Heart Fail. 2011; 4:180–187.
Article8. Rienstra M, Yin X, Larson MG, et al. Relation between soluble ST2, growth differentiation factor-15, and high-sensitivity troponin I and incident atrial fibrillation. Am Heart J. 2014; 167:109–115.e2.
Article9. Dieplinger B, Egger M, Gegenhuber A, Haltmayer M, Mueller T. Analytical and clinical evaluation of a rapid quantitative lateral flow immunoassay for measurement of soluble ST2 in human plasma. Clin Chim Acta. 2015; 451:310–315.
Article10. Neumann T, Vogt J, Schumacher B, et al. Circumferential pulmonary vein isolation with the cryoballoon technique results from a prospective 3-center study. J Am Coll Cardiol. 2008; 52:273–278.11. Andrade JG, Khairy P, Guerra PG, et al. Efficacy and safety of cryoballoon ablation for atrial fibrillation: a systematic review of published studies. Heart Rhythm. 2011; 8:1444–1451.
Article12. Packer DL, Kowal RC, Wheelan KR, et al. Cryoballoon ablation of pulmonary veins for paroxysmal atrial fibrillation: first results of the North American Arctic Front (STOP AF) pivotal trial. J Am Coll Cardiol. 2013; 61:1713–1723.13. Kühne M, Suter Y, Altmann D, et al. Cryoballoon versus radiofrequency catheter ablation of paroxysmal atrial fibrillation: biomarkers of myocardial injury, recurrence rates, and pulmonary vein reconnection patterns. Heart Rhythm. 2010; 7:1770–1776.
Article14. Balk EM, Garlitski AC, Alsheikh-Ali AA, Terasawa T, Chung M, Ip S. Predictors of atrial fibrillation recurrence after radiofrequency catheter ablation: a systematic review. J Cardiovasc Electrophysiol. 2010; 21:1208–1216.
Article15. D'Ascenzo F, Corleto A, Biondi-Zoccai G, et al. Which are the most reliable predictors of recurrence of atrial fibrillation after transcatheter ablation?: a meta-analysis. Int J Cardiol. 2013; 167:1984–1989.16. Boos CJ, Anderson RA, Lip GY. Is atrial fibrillation an inflammatory disorder? Eur Heart J. 2006; 27:136–149.
Article17. Youn JY, Zhang J, Zhang Y, et al. Oxidative stress in atrial fibrillation: an emerging role of NADPH oxidase. J Mol Cell Cardiol. 2013; 62:72–79.
Article18. McMurray JJ, Adamopoulos S, Anker SD, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012; 33:1787–1847.19. Weinberg EO. ST2 protein in heart disease: from discovery to mechanisms and prognostic value. Biomarkers Med. 2009; 3:495–511.
Article20. Miller AM, Liew FY. The IL-33/ST2 pathway--a new therapeutic target in cardiovascular disease. Pharmacol Ther. 2011; 131:179–186.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Soluble ST2 in Paroxysmal Atrial Fibrillation: a New Biomarker that Predicts Recurrence?
- Cryoballoon or Radiofrequency Ablation for Paroxysmal Atrial Fibrillation
- Cryoballoon Ablation for Atrial Fibrillation: a Comprehensive Review and Practice Guide
- Controlled Atrial Fibrillation after Pulmonary Vein Stenting
- A Case of Successful Ablation of Right-Sided Accessory Pathway during Atrial Fibrillation
