Adrenal metastasis in sequentially developed combined hepatocellular carcinoma-cholangiocarcinoma: A case report
- Affiliations
-
- 1Department of Surgery, Seoul National University College of Medicine, Seoul, Korea. Kwleegs@gmail.com
- 2Department of Pathology, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Surgery, Fatmawati General Hospital, Jakarta, Indonesia.
- KMID: 2420619
- DOI: http://doi.org/10.14701/ahbps.2018.22.3.287
Abstract
- The incidence of combined hepatocellular carcinoma-cholangiocarcinoma (cHCC-CC) in a single patient accounts for only 0.4 to 14% of all primary liver cancer. However, the prognosis of its intrahepatic cholangiocarcinoma (ICC) component is poor. We experienced a unique case of a sequentially developed cHCC-CC with adrenal metastasis as the primary presentation and a hidden primary hepatocellular carcinoma. A 65-year-old female with a history of jaundice and abdominal discomfort was diagnosed with S4 ICC measuring 5 cm in diameter, and characterized histologically as papillary adenocarcinoma with intraductal growth, but without any evidence of malignant hepatocyte. S4 segmentectomy with hepaticojejunostomy revealed no additional masses. A follow-up CT scan 3 months after surgery showed a right adrenal mass with markedly increased serum AFP (4950 ng/mL), which was treated with right adrenalectomy. Histopathology revealed a metastatic hepatocellular carcinoma testing positive for AFP, glypican-3, and hepatocytes, but negative for CD-10, inhibin-α, EMA, S-100, and cytokeratin-7. Serum AFP level immediately plummeted to 4.1 ng/mL upon adrenal mass removal. A recurrent S7 liver mass was suspected 1 year later with serum AFP value of 7.6 ng/mL, and characteristic CT imaging of HCC. TACE was performed with good response. Adrenal metastasis may manifest as the primary focus of hepatocellular carcinoma in sequentially developed cHCC-CC patients with hidden primary HCC. cHCC-CC should be considered in the differential diagnosis of cholangiocarcinoma with elevated AFP.
MeSH Terms
Figure
-
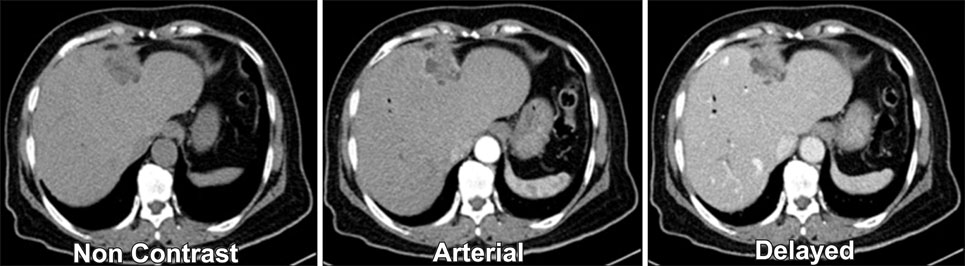
Fig. 1 Initial preoperative CT scan showing a multiple intra-ductal gradually enhancing lesions within the left intrahepatic duct.
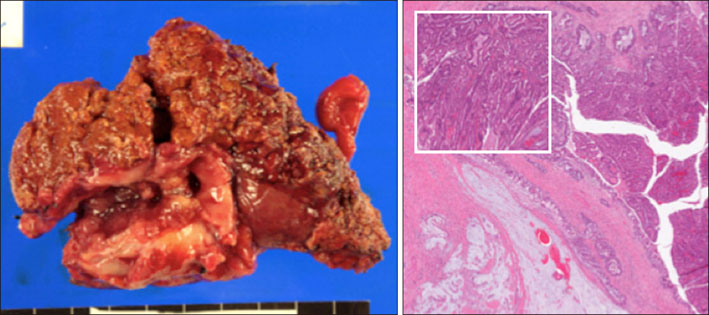
Fig. 2 Liver S4 resection specimen with intraductal tumor infiltration suggesting intrahepatic cholangiocarcinoma.

Fig. 3 Post liver resection imaging studies showing a metastatic right adrenal mass.
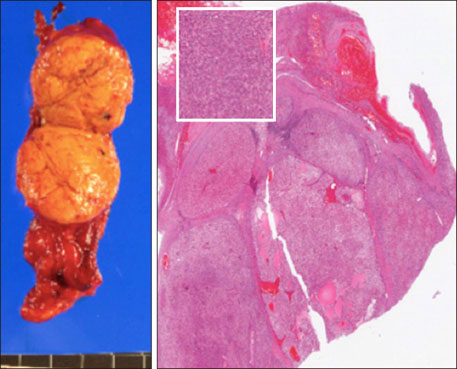
Fig. 4 Metastatic hepatocellular carcinoma of adrenal gland.
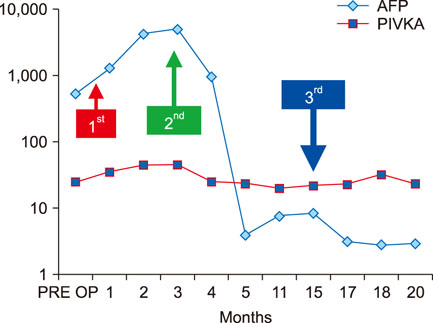
Fig. 5 Levels of AFP (ng/mL) and prothrombin in vitamin K absence II (PIVKA-II) PIVKA-II (mAU/mL) in the disease (logarithmic scale).
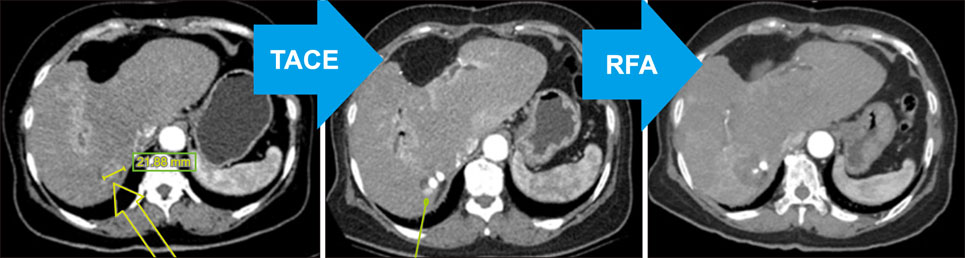
Fig. 6 CT at 15 months post right adrenalectomy showed intrahepateic recurrence near resected right adrenal, 17 months after transarterial chemoembolization (TACE) showed a small viable HCC and 19 months after radiofrequency ablation (RFA) showed no viable HCC.
Reference
-
1. Maximin S, Ganeshan D, Shanbhogue A, Dighe MK, Yeh MM, Kolokythas O, et al. Current update on combined hepatocellular-cholangiocarcinoma. Eur J Radiol Open. 2014; 1:40–48.
Article2. Yap AQ, Chen CL, Yong CC, Kuo FY, Wang SH, Lin CC, et al. Clinicopathological factors impact the survival outcome following the resection of combined hepatocellular carcinoma and cholangiocarcinoma. Surg Oncol. 2013; 22:55–60.3. Park JS, Yoon DS, Kim KS, Choi JS, Lee WJ, Chi HS, et al. What is the best treatment modality for adrenal metastasis from hepatocellular carcinoma? J Surg Oncol. 2007; 96:32–36.
Article4. O'Connor K, Walsh JC, Schaeffer DF. Combined hepatocellular-cholangiocarcinoma (cHCC-CC): a distinct entity. Ann Hepatol. 2014; 13:317–322.5. Allen RA, Lisa JR. Combined liver cell and bile duct carcinoma. Am J Pathol. 1949; 25:647–655.6. Yap AQ, Chen CL, Yong CC, Kuo FY, Wang SH, Lin CC, et al. Clinicopathological factors impact the survival outcome following the resection of combined hepatocellular carcinoma and cholangiocarcinoma. Surg Oncol. 2013; 22:55–60.7. Akiba J, Nakashima O, Hattori S, Tanikawa K, Takenaka M, Nakayama M, et al. Clinicopathologic analysis of combined hepatocellular-cholangiocarcinoma according to the latest WHO classification. Am J Surg Pathol. 2013; 37:496–505.
Article8. Terada T. Combined hepatocellular-cholangiocarcinoma ith stem cell features, ductal plate malformation subtype: a case report and proposal of a new subtype. Int J Clin Exp Pathol. 2013; 6:737–748.9. Lee WS, Lee KW, Heo JS, Kim SJ, Choi SH, Kim YI, et al. Comparison ofcombined hepatocellular and cholangiocarcinoma with hepatocellular carcinoma and intrahepatic cholangiocarcinoma. Surg Today. 2006; 36:892–897.10. Ariizumi S, Kotera Y, KatagiriS , Nakano M, Yamamoto M. Combined hepatocellular-cholangiocarcinoma had poor outcomes after hepatectomy regardless of Allen and Lisa class or the predominance of intrahepatic cholangiocarcinoma cells within the tumors. Ann Surg Oncol. 2012; 19:1628–1636.11. Yasaka K, Gonoi W, Akai H, Katsura M, Akahane M, Kiryu S, et al. Differentiation of adrenal tumors in patients with hepatocellular carcinoma: adrenal adenoma versus metastasis. Eur J Radiol. 2013; 82:1213–1218.
Article12. Chua TC, Morris DL. Exploring the role of resection of extrahepatic metastasis from hepatocellular carcinoma. Surg Oncol. 2012; 21:95–101.13. Park H, Choi KH, Choi SB, Choi JW, Kim DY, Ahn SH, et al. Clinicopathological characteristics in combined hepatocellular-cholangiocarcinoma: a single center study in Korea. Yonsei Med J. 2011; 52:753–760.
Article14. Germain A, Klein M, Brunaud L. Surgical management of adrenal tumors. J Visc Surg. 2011; 148:e250–e261.
Article15. Sancho JJ, Triponez F, Montet X, Sitges-Serra A. Surgical management of adrenal metastases. Langenbecks Arch Surg. 2012; 397:179–194.
Article16. Birsen O, Akyuz M, Dural C, Aksoy E, Aliyev S, Mitchell J, et al. A new risk stratification algorithm for the management of patients with adrenal incidentalomas. Surgery. 2014; 156:959–965.
Article17. Ha TY, Hwang S, Ahn C, Kim KH, Lee YJ, Moon DB, et al. Resection of metachronous adrenal metastasis after liver resection and transplantation for hepatocellular carcinoma. Dig Surg. 2014; 31:428–435.
Article18. Tsalis K, Zacharakis E, Sapidis N, Lambrou I, Zacharakis E, Betsis D. Adrenal metastasis as first presentation of hepatocellular carcinoma. World J Surg Oncol. 2005; 3:50.19. Pandey D, Lee KH, Wong SY, Tan KC. Adrenal metastasis from intrahepatic cholangiocarcinoma. Liver Int. 2007; 27:1016.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Combined Hepatocellular-Cholangiocarcinoma: Recent Progress in Pathology and Classification
- Spontaneous Rupture of Adrenal Metastasis from Hepatocellular Carcinoma
- Adrenal Mass as Initial Presentation of Metastatic Hepatocellular Carcinoma: A Case Report
- Unusual Semimembranosus Muscle Metastasis from Hepatocellular Carcinoma
- Combined Hepatocellular-cholangiocarcinoma
