Surgical Technique for Distal Femur Varization Osteotomy
- Affiliations
-
- 1Department of Orthopedic Surgery, Sahmyook Medical Center, Seoul, Korea. hyw0202@hanmail.net
- 2Department of Orthopedic Surgery, Inje University Ilsan Paik Hospital, Goyang, Korea.
- KMID: 2419465
- DOI: http://doi.org/10.4055/jkoa.2018.53.4.301
Abstract
- A closing wedge distal femoral osteotomy is a procedure to reduce pain and delay the progression of degenerative arthritis of knee by moving the weight bearing line from the lateral compartment to the medial side while preserving the knee joint. Age, weight bearing line, and the degree of arthritis are the essential factors to be considered at the time of surgery. The indications for distal femoral osteotomy are as follows. All patients are aged less than 65 years old, normal medial compartment of the knee with normal patello femoral joint, valgus deformity with lateral degenerative arthritis, younger patients with lateral osteochondritis, congenital osteochondrosis, and recurrent patellar dislocation with genu valgum. The distal femoral osteotomy provides the advantages of rapid pain reduction and short rehabilitation in young and active patients and patients who are subjected to heavy loads on the knee.
MeSH Terms
Figure
-

Figure 1 The mean angle between the lateral femur and the femoral joint is 88°, and the same horizontal line connecting the femur's joint surface and the anatomical axis of the femur. The anatomical lateral distal to retracted angle averages 81°. The MPTA of the tibia between the tibial high pelvic line and the tibial epicondylar axis normally has an average angle of 87° and the medial lateral tibial angle between the ankle line and the tibia is 89° on average. Genu valgum: femur tibia angle >6°–8° weight bearing line >50%. LPFA, lateral proximal femoral angle; mLDFA, mechanical lateral distal femoral angle; JLCA, joint line convergence angle; MPTA, medial proximal tibial angle; LDTA, lateral distal tibial angle.

Figure 2 The distal femoral osteotomy (DFO) must have a closed wedge. Because an open DFO can increase the pressure of the patellar and become dislocated again. Closed DFO reduces the pressure on the patella, making it easier to insert the patella into the joint.
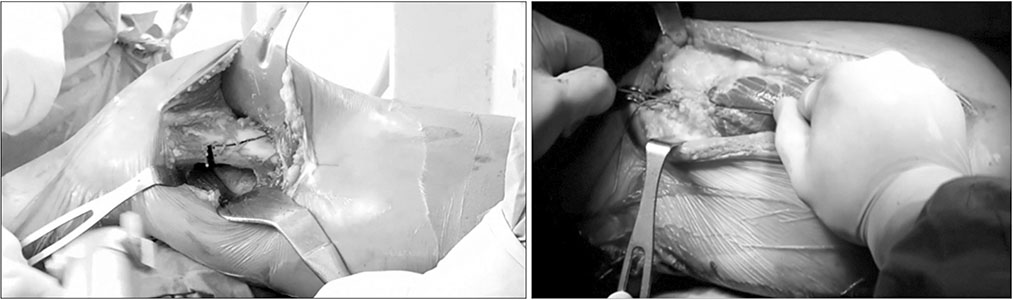
Figure 3 Biplane distal femur osteotomy with medial reefing procedure target point is above the lateral epicondyle of distal femur biplane osteotomy.
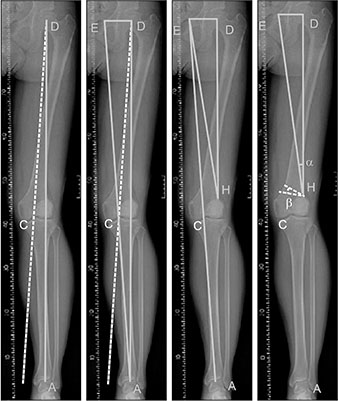
Figure 4 Draw the mechanical axis line AD from the center point ‘A’ of the talus to the center point ‘D’ of the femur head. Draw a new mechanical axis dotted line ‘C’ through the femur center point ‘D’ and a new target line through the target point (most directly inside the tibia medial spine). Raw a line AE from the center point ‘A’ of the talus to the end point ‘E’, where ‘E’ is the same level as the center point ‘D’ of the femur. Draw a line HD from point ‘H’ to the center point ‘D’ of the femur (mostly the lateral cortex of the supracondylar region) and draw the line HE from the hinge point ‘H’ to ‘E’ as well. The angle α between the line HE and line HD formed at this time becomes the size of the angle to be corrected. After β is the same size as α, the osteotomy can be performed by the amount of β produced.

Figure 5 Anterior K-wire (Ø 2.0–2.4 mm) is inserted obliquely in the direction of the above lateral epicondyle beginning at the site to be osteotomized.
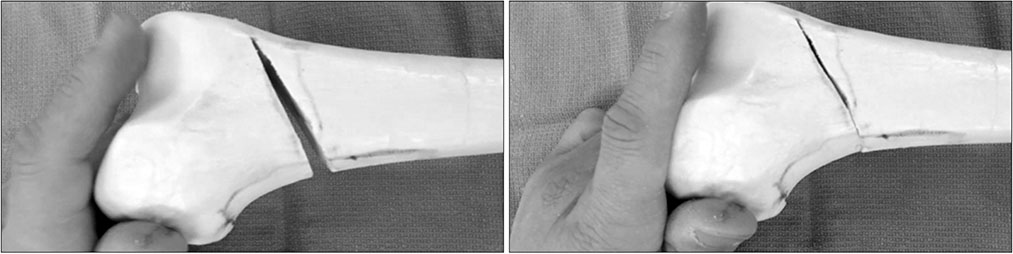
Figure 6 The thickness of the guide pins should be the same for the front (a) and back (b) of the femur (a=b). Therefore, when closed wedge is performed, the space behind will not open. Surgical fracture occurs when a force is applied, so it is important to perform it slowly and repeatedly. After performing a closed wedge, press down on the sole of the foot (after weighing) and check the C-arm for the desired calibration. When fixing the metal plate, check that the metal pin does not enter the intercondylar notch in the proximal femur using a C-arm.
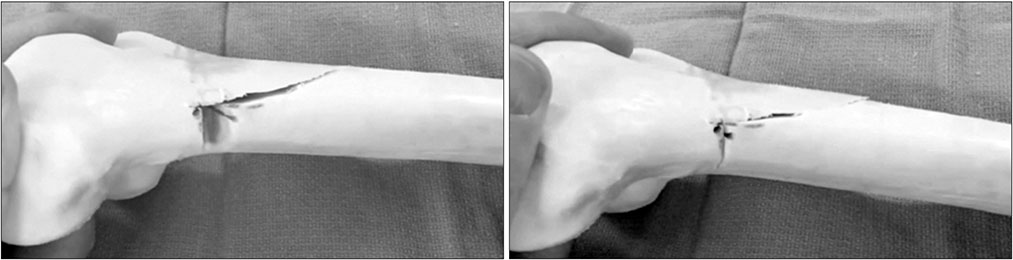
Figure 7 One-third of the anterior femur should be left like a roof, so the K-wire is inserted in the lower 2/3 area of the femur thickness and the osteotomy is performed. The chainsaw to be osteotized is the smallest and thinnest of the osteotomy. In particular, chainsaws should not damage the roof bones.
Reference
-
1. Healy WL, Anglen JO, Wasilewski SA, Krackow KA. Distal femoral varus osteotomy. J Bone Joint Surg Am. 1988; 70:102–109.
Article2. Thein R, Bronak S, Thein R, Haviv B. Distal femoral osteotomy for valgus arthritic knees. J Orthop Sci. 2012; 17:745–749.
Article3. Gross AE, Hutchison CR. Realignment osteotomy of the knee—Part 1: distal femoral varus osteotomy for osteoarthritis of the Valgus knee. Oper Tech Sports Med. 2000; 8:122–126.
Article4. Aglietti P, Menchetti PP. Distal femoral varus osteotomy in the valgus osteoarthritic knee. Am J Knee Surg. 2000; 13:89–95.5. Elahi S, Cahue S, Felson DT, Engelman L, Sharma L. The association between varus-valgus alignment and patellofemoral osteoarthritis. Arthritis Rheum. 2000; 43:1874–1880.
Article6. Shen HC, Chao KH, Huang GS, Pan RY, Lee CH. Combined proximal and distal realignment procedures to treat the habitual dislocation of the patella in adults. Am J Sports Med. 2007; 35:2101–2108.
Article7. Lobenhoffer P, Van Heerwaarden RJ, Staubli AE, Jakob RP. Osteotomies around the knee: indications-planning-surgical techniques using plate fixators. New York: AO Foundation, Thieme;2008. p. 150–152.8. Finkelstein JA, Gross AE, Davis A. Varus osteotomy of the distal part of the femur. A survivorship analysis. J Bone Joint Surg Am. 1996; 78:1348–1352.
Article9. Puddu G, Cipolla M, Cerullo G, Franco V, Giannì E. Which osteotomy for a valgus knee? Int Orthop. 2010; 34:239–247.
Article10. Hunter DJ, Sharma L, Skaife T. Alignment and osteoarthritis of the knee. J Bone Joint Surg Am. 2009; 91:Suppl 1. 85–89.
Article11. Wang JW, Hsu CC. Distal femoral varus osteotomy for osteoarthritis of the knee Surgical technique. J Bone Joint Surg Am. 2006; 88:Suppl 1 Pt 1. 100–108.12. Backstein D, Morag G, Hanna S, Safir O, Gross A. Long-term follow-up of distal femoral varus osteotomy of the knee. J Arthroplasty. 2007; 22:S2–S6.
Article13. Sternheim A, Garbedian S, Backstein D. Distal femoral varus osteotomy: unloading the lateral compartment: long-term follow-up of 45 medial closing wedge osteotomies. Orthopedics. 2011; 34:e488–e490.
Article14. Nelson CL, Saleh KJ, Kassim RA, et al. Total knee arthroplasty after varus osteotomy of the distal part of the femur. J Bone Joint Surg Am. 2003; 85:1062–1065.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Distal Femoral Varization Osteotomy
- Deformity Correction by Femoral Supracondylar Dome Osteotomy with Retrograde Intramedullary Nailing in Varus Deformity of the Distal Femur after Pathologic Fracture of Giant Cell Tumor
- Component Size Matched Extension Gap Osteotomy for TKRA: A New Concept in Knee Osteotomy for TKRA
- Osteotomy around the Knee: Indication and Preoperative Planning
- Surgical Treatment of Habitual Patella Dislocation with Genu Valgum
