Focal Atrial Tachycardia Arising from the Inferior Vena Cava
- Affiliations
-
- 1Department of Cardiology, Yonsei University Health System, Seoul, Korea. hnpak@yuhs.ac
- KMID: 2419099
- DOI: http://doi.org/10.3349/ymj.2017.58.4.884
Abstract
- The inferior vena cava (IVC) is a rare site of focal atrial tachycardia (AT). Here, we report a 20-year-old woman who underwent catheter ablation for anti-arrhythmic drug-resistant AT originating from the IVC. She had undergone open-heart surgery for patch closure of an atrial septal defect 17 years previously and permanent pacemaker implantation for sinus node dysfunction 6 years previously. The AT focus was at the anterolateral aspect of the IVC-right atrial junction, and it was successfully ablated under three-dimensional electroanatomical-mapping guidance. We suspect that the mechanism of this tachycardia was associated with previous IVC cannulation for open-heart surgery.
MeSH Terms
Figure
-
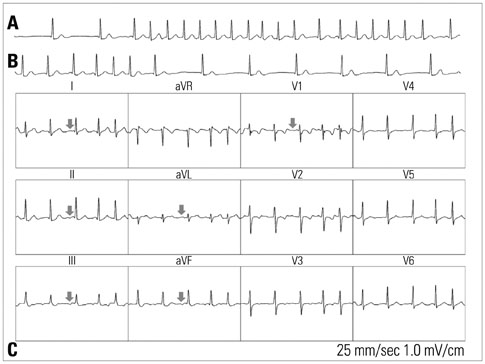
Fig. 1 Electrocardiography (ECG) rhythm strip showing the initiation (A) and termination (B) of clinical atrial tachycardia (AT). The initiation of AT occurs with atrial extrastimuli and terminates abruptly. The patient's basic self-rhythm is junctional rhythm because of sinus node dysfunction after cardiac surgery. A 12-lead ECG of the clinical AT (C).
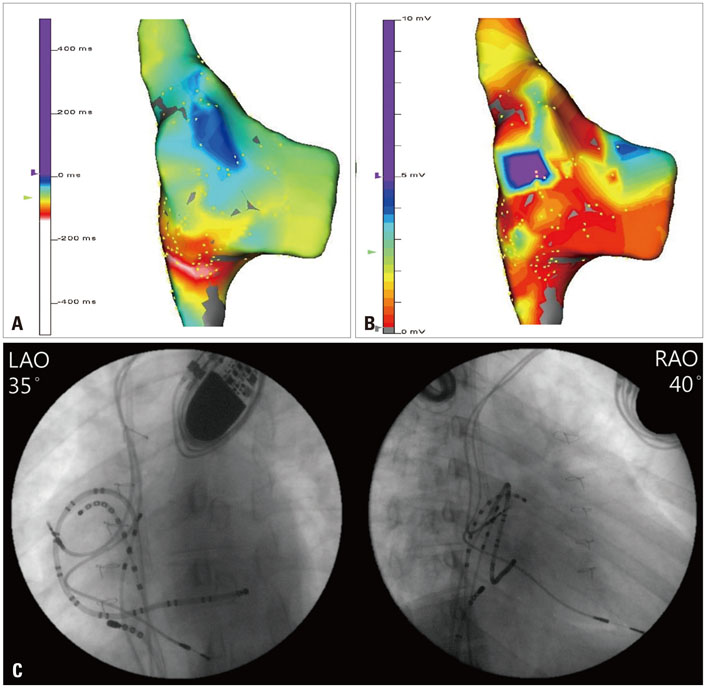
Fig. 2 Three-dimensional (3D) activation map (A). The focal pattern of activation is demonstrated using electroanatomical mapping. The earliest activation site of the tachycardia near the junction between the inferior vena cava (IVC) and right atrium (RA) is shown on the anatomical reconstruction of the RA. The area in white represents the earliest activation region during initiation of the propagation sequence. 3D voltage map (B). Endocardial voltage mapping in the RA is demonstrated. The voltage amplitudes of the sample points (small yellow dots) are assessed, and the points are set to a color scale as indicated in the figure. Large, irregular regions of extremely low voltage (red) consistent with myocardial scarring can be detected over the entire RA. Fluoroscopic projections showing the intracardiac positions of the ablation catheter (C). The catheter ablation site located in the IVC-RA junction is presented in the left anterior oblique view (LAO) and right anterior oblique view (RAO).
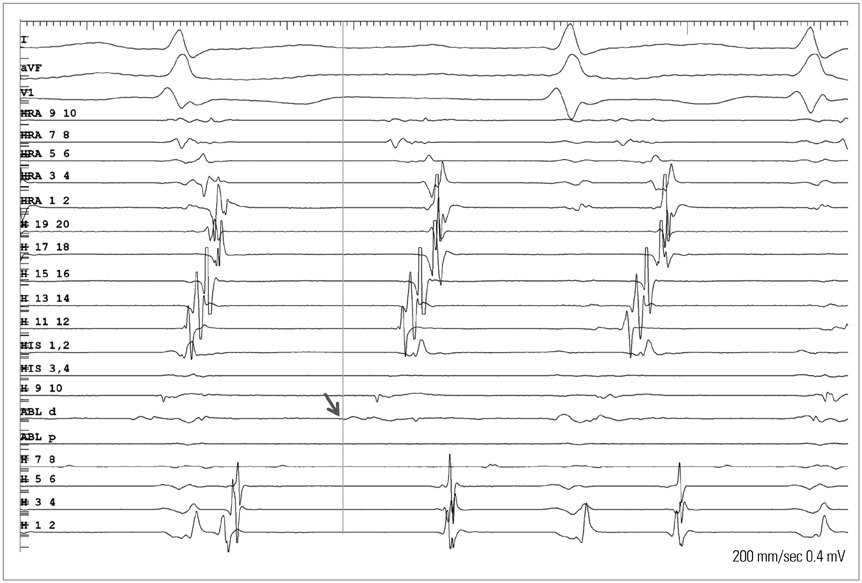
Fig. 3 Intracardiac electrograms and ablation signals at the inferior vena cava, where the local electrogram recorded from the distal electrodes of the ablation catheter during tachycardia preceded the onset of the earliest atrial activation (H9, 10) by 40 ms. ABL, ablation; HRA, high right atrium; HIS, His bundle; H, duodecapolar catheter.
Reference
-
1. de Groot NM, Zeppenfeld K, Wijffels MC, Chan WK, Blom NA, Van der Wall EE, et al. Ablation of focal atrial arrhythmia in patients with congenital heart defects after surgery: role of circumscribed areas with heterogeneous conduction. Heart Rhythm. 2006; 3:526–535.
Article2. Magnin-Poull I, De Chillou C, Miljoen H, Andronache M, Aliot E. Mechanisms of right atrial tachycardia occurring late after surgical closure of atrial septal defects. J Cardiovasc Electrophysiol. 2005; 16:681–687.
Article3. Lukac P, Pedersen AK, Mortensen PT, Jensen HK, Hjortdal V, Hansen PS. Ablation of atrial tachycardia after surgery for congenital and acquired heart disease using an electroanatomic mapping system: Which circuits to expect in which substrate? Heart Rhythm. 2005; 2:64–72.
Article4. Scavée C, Jaïs P, Weerasooriya R, Haïssaguerre M. The inferior vena cava: an exceptional source of atrial fibrillation. J Cardiovasc Electrophysiol. 2003; 14:659–662.5. Yamane T, Miyazaki H, Inada K, Matsuo S, Miyanaga S, Date T, et al. Focal source of atrial fibrillation arising from the ostium of the inferior vena cava. Circ J. 2005; 69:756–759.
Article6. Kato Y, Horigome H, Takahashi-Igari M, Aonuma K. Focal atrial tachycardia originating from inside the inferior vena cava late after surgical repair of congenital heart defects. Pediatr Cardiol. 2011; 32:846–848.
Article7. Higa S, Tai CT, Lin YJ, Liu TY, Lee PC, Huang JL, et al. Focal atrial tachycardia: new insight from noncontact mapping and catheter ablation. Circulation. 2004; 109:84–91.
Article8. Katsivas AG, Manolis AG, Vassilopoulos C, Ioanidis P, Giotopoulou A, Kyriakides Z. Electroanatomical mapping of a right atrial tachycardia originating within the inferior vena cava. Hellenic J Cardiol. 2004; 45:187–190.9. Murphy JG, Gersh BJ, McGoon MD, Mair DD, Porter CJ, Ilstrup DM, et al. Long-term outcome after surgical repair of isolated atrial septal defect. Follow-up at 27 to 32 years. N Engl J Med. 1990; 323:1645–1650.
Article10. Pap R, Kohári M, Makai A, Bencsik G, Traykov VB, Gallardo R, et al. Surgical technique and the mechanism of atrial tachycardia late after open heart surgery. J Interv Card Electrophysiol. 2012; 35:127–135.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transposition of inferior vena cava
- A case of hemiazygos continuation of a left inferior vena cava
- Leiomyosarcoma arising from the inferior vena cava: a case report
- Persistent Left Superior Vena Cava with Absent Right Superior Vena Cava and Large Atrial Septal Defect in Visceroatrial Situs solitus
- Obstruction of the Hepatic Portion of the Inferior Vena Cava
