Coronary Artery Vasospasm
- Affiliations
-
- 1Department of Cardiology, Asan Medical Center Heart Institute, University of Ulsan College of Medicine, Seoul, Korea. jksong@amc.seoul.kr
- KMID: 2418803
- DOI: http://doi.org/10.4070/kcj.2018.0251
Abstract
- Coronary artery vasospasm (CVS) is an important mechanism of myocardial ischemia and produces any of the manifestations of coronary artery disease from silent myocardial ischemia, to effort-induced angina and variant angina, to acute coronary syndrome including myocardial infarction or sudden cardiac death. The pathogenesis, characteristic clinical features, diagnosis, and treatment of CVS are summarized. Emphasis is placed on correct diagnosis of CVS using pharmacological spasm provocation test, either during coronary angiography or with echocardiographic monitoring of ventricular wall motion. Current underutilization of pharmacologic provocative test at the time of coronary angiography cannot be justified, as there is no evidence supporting that the incidence of CVS is declining. Physicians' vigilance for objective documentation of CVS is necessary for appropriate management of patients with various clinical presentations of ischemic heart disease.
Keyword
MeSH Terms
Figure
-
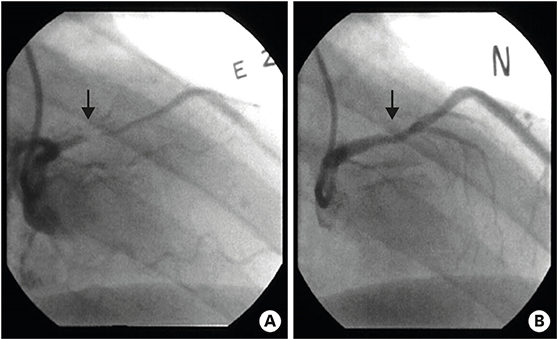
Figure 1 A representative case of coronary artery vasospasm documented by pharmacologic spasm provocation test during invasive coronary angiography: focal vasoconstriction (arrow, A) resulting in total occlusion of proximal left anterior descending coronary artery developed with ergonovine injection (E2, A), which was normalized with nitroglycerin administration (N, B).
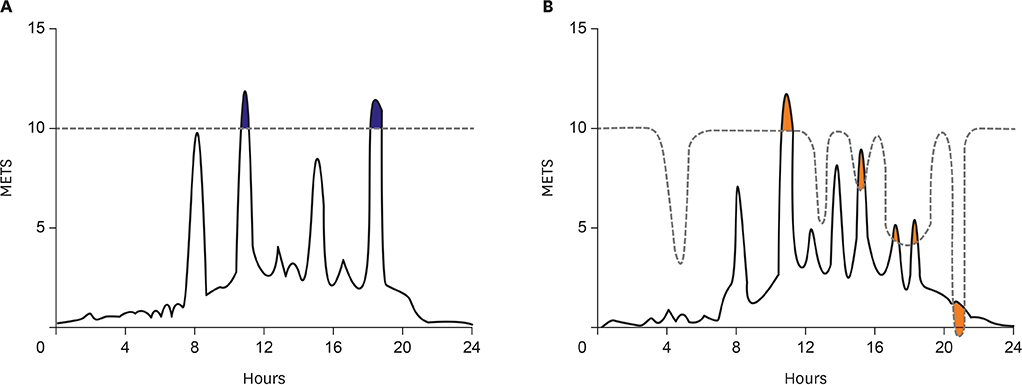
Figure 2 Schematic illustrations showing relationship between angina threshold (dotted line) and daily activity in classic effort angina (A) and variant angina (B). In classic effort angina with fixed angina threshold, daily activity exceeding the angina threshold results in chest pain attack (blue), which is quite predictable and usually develops during daytime paralleling with the level of physical activity. However, in variant angina, the angina threshold itself varies significantly during a day and the level of physical activity is not associated with chest pain attack: thus, chest pain attack is quite unpredictable depending on the change of angina threshold, not on the level of physical activity (orange) (modified from reference 3). METS = metabolic equivalents.

Figure 3 A representative Holter monitoring in a patient with spontaneous coronary vasospasm. Characteristic ST-segment elevation at early morning with rapid progression to ventricular tachyarrhythmia is well demonstrated.
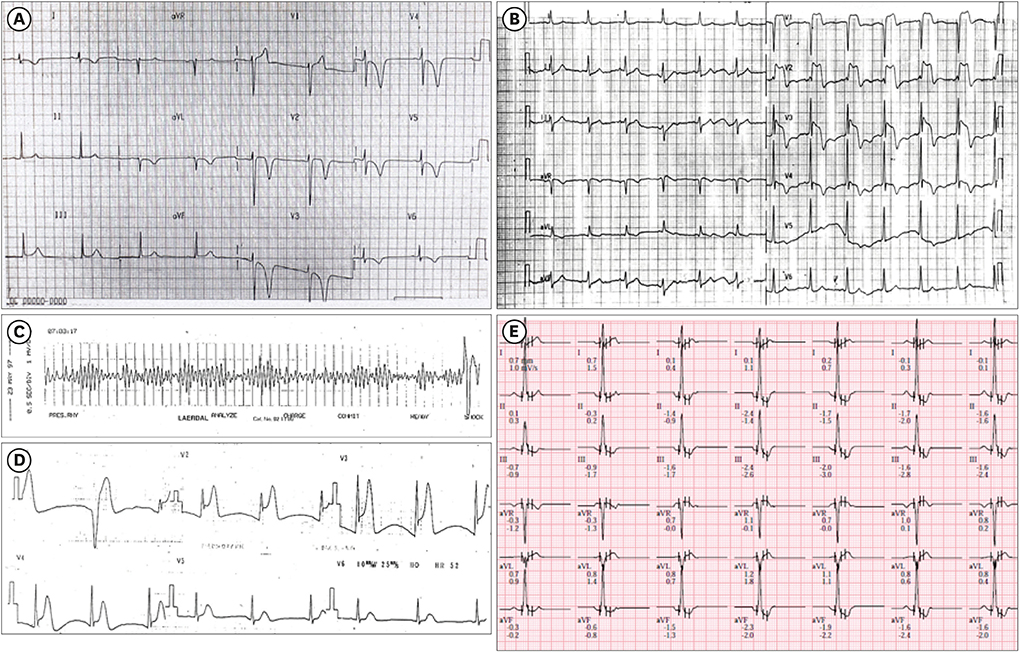
Figure 4 Representative electrocardiograms showing various clinical presentations of patients with coronary artery vasospasm: acute coronary syndrome with deep T wave inversion in the precordial leads (A), prominent ST-segment elevation mimicking ST elevation myocardial infarction (B), development of ventricular fibrillation and ST elevation in aborted sudden cardiac death (C, D), and ST-segment depression during exercise treadmill test in a patient with effort-induced chest pain (E).

Figure 5 Serial coronary angiograms in a patient who developed coronary artery vasospasm after repeated interventions for fixed stenosis of the left anterior descending coronary artery.
Cited by 1 articles
-
Coronary Spasm during General Anesthesia in a Patient with Previously Undiagnosed Variant Angina
Gi year Lee, Sooyoung Cho, Dong Yeon Kim, Seung Hee Yoo
Ewha Med J. 2022;45(4):e17. doi: 10.12771/emj.2022.e17.
Reference
-
1. Prinzmetal M, Kennamer R, Merliss R, Wada T, Bor N. Angina pectoris. I. A variant form of angina pectoris; preliminary report. Am J Med. 1959; 27:375–388.2. Oliva PB, Potts DE, Pluss RG. Coronary arterial spasm in Prinzmetal angina. Documentation by coronary arteriography. N Engl J Med. 1973; 288:745–751.3. Maseri A. Louis F. Bishop lecture. Role of coronary artery spasm in symptomatic and silent myocardial ischemia. J Am Coll Cardiol. 1987; 9:249–262.4. Heupler FA Jr, Proudfit WL, Razavi M, Shirey EK, Greenstreet R, Sheldon WC. Ergonovine maleate provocative test for coronary arterial spasm. Am J Cardiol. 1978; 41:631–640.
Article5. Yasue H, Horio Y, Nakamura N, et al. Induction of coronary artery spasm by acetylcholine in patients with variant angina: possible role of the parasympathetic nervous system in the pathogenesis of coronary artery spasm. Circulation. 1986; 74:955–963.
Article6. Hackett D, Larkin S, Chierchia S, Davies G, Kaski JC, Maseri A. Induction of coronary artery spasm by a direct local action of ergonovine. Circulation. 1987; 75:577–582.
Article7. Park SW, Park SJ, Kim JJ, Song JK, Seong IW, Lee JK. A comparative study of acetylcholine and ergonovine provocative test in patients with chest pain syndrome with normal or near normal coronary arteriograms. Korean Circ J. 1991; 21:842–848.
Article8. Zaya M, Mehta PK, Merz NB. Provocative testing for coronary reactivity and spasm. J Am Coll Cardiol. 2014; 63:103–109.9. MacAlpin RN. Some observations on and controversies about coronary arterial spasm. Int J Cardiol. 2015; 181:389–398.
Article10. Beltrame JF, Crea F, Kaski JC, et al. International standardization of diagnostic criteria for vasospastic angina. Eur Heart J. 2017; 38:2565–2568.
Article11. Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2012; 60:e44–164.12. Anderson JL, Adams CD, Antman EM, et al. 2012 ACCF/AHA focused update incorporated into the ACCF/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013; 61:e179–347.13. JCS Joint Working Group. Guidelines for diagnosis and treatment of patients with vasospastic angina (Coronary Spastic Angina) (JCS 2013). Circ J. 2014; 78:2779–2801.14. Yasue H, Nagao M, Omote S, Takizawa A, Miwa K, Tanaka S. Coronary arterial spasm and Prinzmetal’s variant form of angina induced by hyperventilation and Tris-buffer infusion. Circulation. 1978; 58:56–62.
Article15. Waters DD, Szlachcic J, Bonan R, Miller DD, Dauwe F, Theroux P. Comparative sensitivity of exercise, cold pressor and ergonovine testing in provoking attacks of variant angina in patients with active disease. Circulation. 1983; 67:310–315.
Article16. Bertrand ME, LaBlanche JM, Tilmant PY, et al. Frequency of provoked coronary arterial spasm in 1089 consecutive patients undergoing coronary arteriography. Circulation. 1982; 65:1299–1306.
Article17. Takagi Y, Yasuda S, Takahashi J, et al. Clinical implications of provocation tests for coronary artery spasm: safety, arrhythmic complications, and prognostic impact: multicentre registry study of the Japanese Coronary Spasm Association. Eur Heart J. 2013; 34:258–267.
Article18. Song JK, Park SW, Kim JJ, et al. Values of intravenous ergonovine test with two-dimensional echocardiography for diagnosis of coronary artery spasm. J Am Soc Echocardiogr. 1994; 7:607–615.
Article19. Song JK, Lee SJ, Kang DH, et al. Ergonovine echocardiography as a screening test for diagnosis of vasospastic angina before coronary angiography. J Am Coll Cardiol. 1996; 27:1156–1161.
Article20. Djordjevic-Dikic A, Varga A, Rodriguez O, et al. Safety of ergotamine-ergic pharmacologic stress echocardiography for vasospasm testing in the echo lab: 14 year experience on 478 tests in 464 patients. Cardiologia. 1999; 44:901–906.21. Song JK, Park SW, Kang DH, et al. Safety and clinical impact of ergonovine stress echocardiography for diagnosis of coronary vasospasm. J Am Coll Cardiol. 2000; 35:1850–1856.
Article22. Buxton A, Goldberg S, Hirshfeld JW, et al. Refractory ergonovine-induced coronary vasospasm: importance of intracoronary nitroglycerin. Am J Cardiol. 1980; 46:329–334.
Article23. Nesto RW, Kowalchuck GJ. The ischemic cascade: temporal sequence of hemodynamic, electrocardiographic and symptomatic expressions of ischemia. Am J Cardiol. 1987; 59:23C–30C.
Article24. Yasue H, Takizawa A, Nagao M, et al. Long-term prognosis for patients with variant angina and influential factors. Circulation. 1988; 78:1–9.
Article25. Ahn JM, Lee KH, Yoo SY, et al. Prognosis of variant angina manifesting as aborted sudden cardiac death. J Am Coll Cardiol. 2016; 68:137–145.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Native Coronary Artery and Grafted Artery Spasm Just after Coronary Artery Bypass Grafting: A Case Report
- A case of coronary vasospasm-induced ventricular fibrillation without significant coronary artery disease
- Coronary Artery Vasospasm with Acute Myocarditis in an Adolescent
- Intercoronary Communication between the Circumflex and Right Coronary Arteries Coexisted with Coronary Vasospasm
- Chest Pain due to Coronary Artery Vasospasm after Aortic Valve Replacement Surgery: A case report
