Yonsei Med J.
2018 Mar;59(2):258-264. 10.3349/ymj.2018.59.2.258.
Comparison of Rhythm and Rate Control Strategies for Stroke Occurrence in a Prospective Cohort of Atrial Fibrillation Patients
- Choi YJ

- Kang KW
- Kim TH
- Cha MJ
- Lee JM
- Park J
- Park JK
- Shim J
- Uhm JS
- Kim J
- Park HW
- Choi EK
- Kim JB
- Kim C
- Lee YS
- Joung B
- Affiliations
-
- 1Division of Cardiology, Eulji University Hospital, Eulji University College of Medicine, Daejeon, Korea. kwkang@eulji.ac.kr
- 2Division of Cardiology, Department of Internal Medicine, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea. cby6908@yuhs.ac
- 3Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
- 4Division of Cardiology, Department of Internal Medicine, Kyung Hee University Hospital, Kyung Hee University, Seoul, Korea.
- 5Department of Cardiology, School of Medicine, Ewha Womans University, Seoul, Korea.
- 6Department of Cardiology, Hanyang University Seoul Hospital, Seoul, Korea.
- 7Division of Cardiology, Department of Internal Medicine, Korea University Medical Center, Seoul, Korea.
- 8Heart Institute, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 9Department of Cardiology, Chonnam National University Hospital, Chonnam National University Medical School, Gwangju, Korea.
- 10Department of Preventive Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 11Division of Cardiology, Department of Internal Medicine, Daegu Catholic University Medical Center, Daegu, Korea.
- KMID: 2418789
- DOI: http://doi.org/10.3349/ymj.2018.59.2.258
Abstract
- PURPOSE
Comparisons of rhythm and rate control strategies for stroke prevention in patients with atrial fibrillation (AF) are still inconclusive. We compared differences in clinical outcomes between the rhythm and rate control strategies.
MATERIALS AND METHODS
The COmparison study of Drugs for symptom control and complication prEvention of Atrial Fibrillation (CODE-AF) registry prospectively enrolled 6000 patients who were treated for AF using real-world guideline adherence at multiple referral centers. In total, 2508 (41.8%) patients were clinically followed up for over six months. Of these, 1134 (45.2 %) patients treated by rhythm control and 1374 (54.8 %) patients treated by rate control were analyzed for clinical outcomes, including stroke and cardiovascular outcomes.
RESULTS
Among all patients (age, 68±10 years; male, 62.4%), those treated with the rhythm control strategy were significantly younger, had more symptomatic paroxysmal AF, and a shorter AF duration, and were less likely to have diabetes, renal dysfunction, and heart failure, compared to those treated with the rate control strategy (CHAâ‚‚DSâ‚‚-VASc score 2.4±1.5 vs. 3.1±1.7, p < 0.001). Even though oral anticoagulation was similarly prescribed in both groups, occurrence of stroke was less likely to occur in the rhythm control strategy group (0.0% vs. 0.7%, p=0.015). Multivariate Cox hazard regression showed that only age, especially more than 75 years old, were significantly correlated with the occurrence of stroke, regardless of the strategy used for treatment.
CONCLUSION
In this prospective AF cohort, compared with the rate control strategy, the rhythm control strategy was associated with fewer cardiovascular events and strokes in a short-term period.
Keyword
MeSH Terms
-
Administration, Oral
Aged
Antithrombins/administration & dosage/therapeutic use
Atrial Fibrillation/drug therapy/*physiopathology
Female
Heart Rate/*physiology
Humans
Kaplan-Meier Estimate
Male
Proportional Hazards Models
Prospective Studies
Stroke/drug therapy/*etiology/*physiopathology
Treatment Outcome
Antithrombins
Figure
-
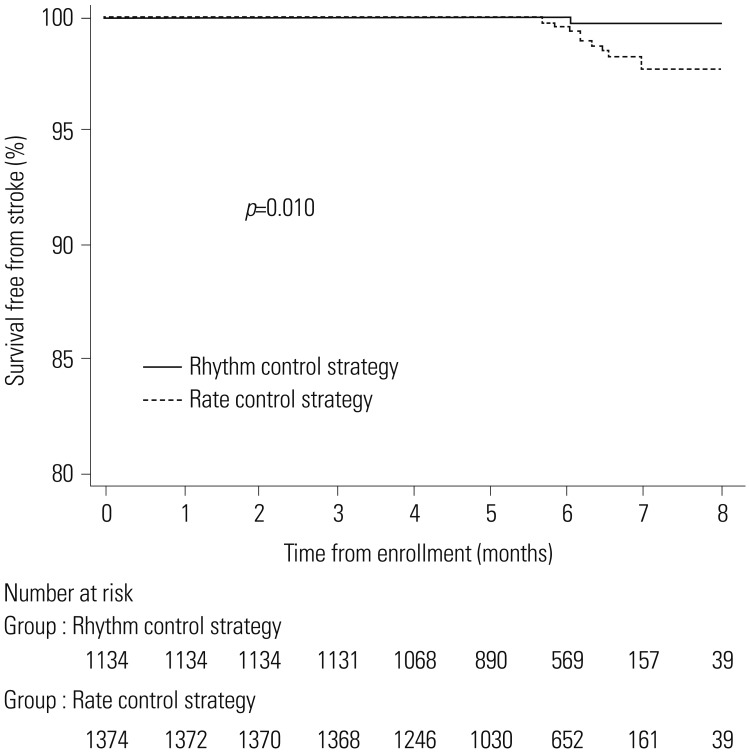
Fig. 1 Kaplan-Meier survival curve showing the comparison of the rhythm and rate control strategies for stroke occurrence.
Cited by 2 articles
-
2018 Korean Guideline of Atrial Fibrillation Management
Boyoung Joung, Jung Myung Lee, Ki Hong Lee, Tae-Hoon Kim, Eue-Keun Choi, Woo-Hyun Lim, Ki-Woon Kang, Jaemin Shim, Hong Euy Lim, Junbeom Park, So-Ryoung Lee, Young Soo Lee, Jin-Bae Kim,
Korean Circ J. 2018;48(12):1033-1080. doi: 10.4070/kcj.2018.0339.Cost-Effectiveness of Rate- and Rhythm-Control Drugs for Treating Atrial Fibrillation in Korea
Min Kim, Woojin Kim, Changsoo Kim, Boyoung Joung
Yonsei Med J. 2019;60(12):1157-1163. doi: 10.3349/ymj.2019.60.12.1157.
Reference
-
1. Bunch TJ, Crandall BG, Weiss JP, May HT, Bair TL, Osborn JS, et al. Patients treated with catheter ablation for atrial fibrillation have long-term rates of death, stroke, and dementia similar to patients without atrial fibrillation. J Cardiovasc Electrophysiol. 2011; 22:839–845. PMID: 21410581.
Article2. Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016; 37:2893–2962. PMID: 27567408.
Article3. January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014; 130:e199–e267. PMID: 24682347.
Article4. Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007; 146:857–867. PMID: 17577005.
Article5. Freedman B, Potpara TS, Lip GY. Stroke prevention in atrial fibrillation. Lancet. 2016; 388:806–817. PMID: 27560276.
Article6. Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz MD, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014; 383:955–962. PMID: 24315724.
Article7. Rolf S, Kornej J, Dagres N, Hindricks G. What can rhythm control therapy contribute to prognosis in atrial fibrillation? Heart. 2015; 101:842–846. PMID: 25792720.
Article8. Al-Khatib SM, Allen LaPointe NM, Chatterjee R, Crowley MJ, Dupre ME, Kong DF, et al. Rate- and rhythm-control therapies in patients with atrial fibrillation: a systematic review. Ann Intern Med. 2014; 160:760–773. PMID: 24887617.9. Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002; 347:1825–1833. PMID: 12466506.
Article10. Scheinman MM. Atrial fibrillation therapy: rate versus rhythm control. Pacing Clin Electrophysiol. 2003; 26:1175–1177. PMID: 12765444.11. Gillinov AM, Bagiella E, Moskowitz AJ, Raiten JM, Groh MA, Bowdish ME, et al. Rate control versus rhythm control for atrial fibrillation after cardiac surgery. N Engl J Med. 2016; 374:1911–1921. PMID: 27043047.
Article12. Tsadok MA, Jackevicius CA, Essebag V, Eisenberg MJ, Rahme E, Humphries KH, et al. Rhythm versus rate control therapy and subsequent stroke or transient ischemic attack in patients with atrial fibrillation. Circulation. 2012; 126:2680–2687. PMID: 23124034.
Article13. Bunch TJ, May HT, Bair TL, Weiss JP, Crandall BG, Osborn JS, et al. Atrial fibrillation ablation patients have long-term stroke rates similar to patients without atrial fibrillation regardless of CHADS2 score. Heart Rhythm. 2013; 10:1272–1277. PMID: 23835257.
Article14. Stevens PE, Levin A. Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013; 158:825–830. PMID: 23732715.
Article15. January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014; 64:e1–e76. PMID: 24685669.16. Calkins H, Brugada J, Packer DL, Cappato R, Chen SA, Crijns HJ, et al. HRS/EHRA/ECAS expert Consensus Statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2007; 4:816–861. PMID: 17556213.
Article17. Kim H, Kim TH, Cha MJ, Lee JM, Park J, Park JK, et al. A Prospective survey of atrial fibrillation management for real-world guideline adherence: COmparison study of Drugs for symptom control and complication prEvention of Atrial Fibrillation (CODE-AF) Registry. Korean Circ J. 2017; 47:877–887. PMID: 29171211.
Article18. Schulman S, Kearon C. Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost. 2005; 3:692–694. PMID: 15842354.
Article19. Kaatz S, Ahmad D, Spyropoulos AC, Schulman S. Subcommittee on Control of Anticoagulation. Definition of clinically relevant non-major bleeding in studies of anticoagulants in atrial fibrillation and venous thromboembolic disease in non-surgical patients: communication from the SSC of the ISTH. J Thromb Haemost. 2015; 13:2119–2126. PMID: 26764429.
Article20. Hohnloser SH, Kuck KH, Lilienthal J. Rhythm or rate control in atrial fibrillation--Pharmacological Intervention in Atrial Fibrillation (PIAF): a randomised trial. Lancet. 2000; 356:1789–1794. PMID: 11117910.
Article21. Hagens VE, Vermeulen KM, TenVergert EM, TenVergert DJ, Bosker HA, Kamp O, et al. Rate control is more cost-effective than rhythm control for patients with persistent atrial fibrillation--results from the RAte Control versus Electrical cardioversion (RACE) study. Eur Heart J. 2004; 25:1542–1549. PMID: 15342174.
Article22. Chatterjee S, Sardar P, Lichstein E, Mukherjee D, Aikat S. Pharmacologic rate versus rhythm-control strategies in atrial fibrillation: an updated comprehensive review and meta-analysis. Pacing Clin Electrophysiol. 2013; 36:122–133. PMID: 22978656.
Article23. Shin DG, Cho I, Hartaigh Bó, Mun HS, Lee HY, Hwang ES, et al. Cardiovascular events of electrical cardioversion under optimal anticoagulation in atrial fibrillation: the multicenter analysis. Yonsei Med J. 2015; 56:1552–1558. PMID: 26446636.
Article24. Saliba W, Schliamser JE, Lavi I, Barnett-Griness O, Gronich N, Rennert G. Catheter ablation of atrial fibrillation is associated with reduced risk of stroke and mortality: a propensity score-matched analysis. Heart Rhythm. 2017; 14:635–642. PMID: 28189823.
Article25. Camm AJ, Breithardt G, Crijns H, Dorian P, Kowey P, Le Heuzey JY, et al. Real-life observations of clinical outcomes with rhythm- and rate-control therapies for atrial fibrillation RECORDAF (Registry on Cardiac Rhythm Disorders Assessing the Control of Atrial Fibrillation). J Am Coll Cardiol. 2011; 58:493–501. PMID: 21777747.26. Sherman DG. Stroke prevention in atrial fibrillation: pharmacological rate versus rhythm control. Stroke. 2007; 38(2 Suppl):615–617. PMID: 17261701.27. Suzuki S, Yamashita T, Okumura K, Atarashi H, Akao M, Ogawa H, et al. Incidence of ischemic stroke in Japanese patients with atrial fibrillation not receiving anticoagulation therapy--pooled analysis of the Shinken Database, J-RHYTHM Registry, and Fushimi AF Registry. Circ J. 2015; 79:432–438. PMID: 25501800.28. Steinberg BA, Holmes DN, Ezekowitz MD, Fonarow GC, Kowey PR, Mahaffey KW, et al. Rate versus rhythm control for management of atrial fibrillation in clinical practice: results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) registry. Am Heart J. 2013; 165:622–629. PMID: 23537981.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Mechanism of and Preventive Therapy for Stroke in Patients with Atrial Fibrillation
- Optimal Rhythm Control Strategy in Patients With Atrial Fibrillation
- Spontaneous Conversion of Atrial Fibrillation to Normal Sinus Rhythm Following Recurrent Cerebral Infarctions
- How and When to Screen for Atrial Fibrillation after Stroke: Insights from Insertable Cardiac Monitoring Devices
- Catheter Ablation of Long-standing Persistent Atrial Fibrillation: a Reckless Challenge or a Way to Real Cure?
