Korean J Radiol.
2018 Oct;19(5):866-871. 10.3348/kjr.2018.19.5.866.
2018 Korean Clinical Imaging Guideline for Hemoptysis
- Affiliations
-
- 1Department of Radiolgoy, InJe University Sanggye Paik Hospital, Seoul 01757, Korea.
- 2Department of Radiology, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon 35015, Korea.
- 3Department of Radiology, Gachon University Gil Hospital, Incheon 21565, Korea.
- 4Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 05505, Korea.
- 5Department of Radiology, Kyungpook National University Medical Center, Daegu 41944, Korea.
- 6Department of Radiology, Kyung Hee University Hospital at Gangdong, Kyung Hee University College of Medicine, Seoul 05278, Korea.
- 7Department of Radiology, Seoul National University Hospital, Seoul 03080, Korea.
- 8Department of Radiology, Korea University Guro Hospital, Korea University College of Medicine, Seoul 08308, Korea.
- 9Division for Healthcare Technology Assessment Research, National Evidence-based Healthcare Collaborating Agency, Seoul 04554, Korea.
- 10Department of Radiology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul 06591, Korea. jijung@catholic.ac.kr
- KMID: 2418549
- DOI: http://doi.org/10.3348/kjr.2018.19.5.866
Abstract
- In 2014, the American College of Radiology (ACR) announced the guideline for the appropriate diagnostic approach and treatment of patients according to the severity of hemoptysis and risk for lung cancer. However, the application of the ACR guideline in Korea may not be appropriate, because many patients in Korea have active tuberculosis or pulmonary fibrosis due to previous tuberculosis. The Korean Society of Radiology and Korean Society of Thoracic Radiology have proposed a new guideline suitable for Korean practice. This new guideline was prepared through the consensus of a development committee, working party, and an advisory committee. The guideline proposal process was based on an evidence-based clinical imaging guideline proposed by the development committee. Clinical imaging guideline for adult patients with hemoptysis is as follows: Chest radiography is an initial imaging modality to evaluate hemoptysis. Contrast-enhanced chest CT is recommended in patients with two risk factors for lung cancer (> 40 years old and > 30 pack-year smoking history), moderate hemoptysis (> 30 mL/24 hours) or recurrent hemoptysis. Contrast-enhanced chest CT is also recommended in patients with massive hemoptysis (> 400 mL/24 hours) without cardiopulmonary compromise.
Keyword
MeSH Terms
Figure
-
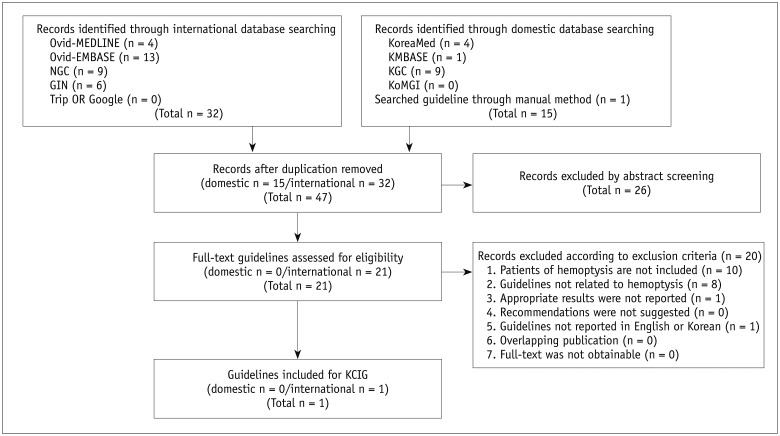
Fig. 1 Flow chart for literature selection.GIN = Guideline International Network, KCIG = Korean Clinical Imaging Guidelines, KGC = Korean Guideline Clearinghouse, KoMGI = Korean Medical Guidelines and Information, NGC = National Guideline Clearinghouse
Cited by 1 articles
-
Guidelines for Transrectal Ultrasonography-Guided Prostate Biopsy: Korean Society of Urogenital Radiology Consensus Statement for Patient Preparation, Standard Technique, and Biopsy-Related Pain Management
Myoung Seok Lee, Min Hoan Moon, Chan Kyo Kim, Sung Yoon Park, Moon Hyung Choi, Sung Il Jung,
Korean J Radiol. 2020;21(4):422-430. doi: 10.3348/kjr.2019.0576.
Reference
-
1. ACR Appropriateness Criteria®. Hemoptysis. American College of Radiology Web site. Accessed January 31, 2017. https://acsearch.acr.org/docs/69449/Narrative/. Published August, 2010.2. Choi SJ, Jeong WK, Jo AJ, Choi JA, Kim MJ, Lee M, et al. Methodology for developing evidence-based clinical imaging guidelines: joint recommendations by Korean Society of Radiology and National Evidence-Based Healthcare Collaborating Agency. Korean J Radiol. 2017; 18:208–216. PMID: 28096730.
Article3. Tsoumakidou M, Chrysofakis G, Tsiligianni I, Maltezakis G, Siafakas NM, Tzanakis N. A prospective analysis of 184 hemoptysis cases: diagnostic impact of chest X-ray, computed tomography, bronchoscopy. Respiration. 2006; 73:808–814. PMID: 16446530.4. Fidan A, Ozdoğan S, Oruç O, Salepçi B, Ocal Z, Cağlayan B. Hemoptysis: a retrospective analysis of 108 cases. Respir Med. 2002; 96:677–680. PMID: 12243312.
Article5. Bruzzi JF, Rémy-Jardin M, Delhaye D, Teisseire A, Khalil C, Rémy J. Multi-detector row CT of hemoptysis. Radiographics. 2006; 26:3–22. PMID: 16418239.
Article6. Lee SJ, Rho JY, Yoo SM, Kim MD, Lee JH, Kim EK, et al. Usefulness of multi-detector computed tomography before bronchoscopy and/or bronchial arterial embolization for hemoptysis. Tuberc Respir Dis. 2010; 68:80–86.
Article7. Revel MP, Fournier LS, Hennebicque AS, Cuenod CA, Meyer G, Reynaud P, et al. Can CT replace bronchoscopy in the detection of the site and cause of bleeding in patients with large or massive hemoptysis? AJR Am J Roentgenol. 2002; 179:1217–1224. PMID: 12388502.
Article8. Delage A, Tillie-Leblond I, Cavestri B, Wallaert B, Marquette CH. Cryptogenic hemoptysis in chronic obstructive pulmonary disease: characteristics and outcome. Respiration. 2010; 80:387–392. PMID: 19996573.
Article9. Menchini L, Remy-Jardin M, Faivre JB, Copin MC, Ramon P, Matran R, et al. Cryptogenic haemoptysis in smokers: angiography and results of embolisation in 35 patients. Eur Respir J. 2009; 34:1031–1039. PMID: 19357153.
Article10. Poe RH, Israel RH, Marin MG, Ortiz CR, Dale RC, Wahl GW, et al. Utility of fiberoptic bronchoscopy in patients with hemoptysis and a nonlocalizing chest roentgenogram. Chest. 1988; 93:70–75. PMID: 3335170.
Article11. Herth F, Ernst A, Becker HD. Long-term outcome and lung cancer incidence in patients with hemoptysis of unknown origin. Chest. 2001; 120:1592–1594. PMID: 11713139.
Article12. Thirumaran M, Sundar R, Sutcliffe IM, Currie DC. Is investigation of patients with haemoptysis and normal chest radiograph justified? Thorax. 2009; 64:854–856. PMID: 19457872.
Article13. McGuinness G, Beacher JR, Harkin TJ, Garay SM, Rom WN, Naidich DP. Hemoptysis: prospective high-resolution CT/bronchoscopic correlation. Chest. 1994; 105:1155–1162. PMID: 8162743.
Article14. Kim HB. Bronchial artery embolization. Korean Society of Interventional Radiology. Interventional radiology. 2nd ed. Seoul: Ilchokak;2014. p. 321–325.15. Millar AB, Boothroyd AE, Edwards D, Hetzel MR. The role of computed tomography (CT) in the investigation of unexplained haemoptysis. Respir Med. 1992; 86:39–44. PMID: 1565816.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Korean Clinical Imaging Guideline for Hemoptysis
- The Causes and Clinical Course of Massive Hemoptysis
- Recurrent hemoptysis in a 26-year-old woman with a ground-glass opacity lesion of the lung
- Breast Magnetic Resonance Image (MRI) Guideline: Breast Imaging Study Group of Korean Society of Magnetic Resonance in Medicine Recommendations
- Optimal time to localize bleeding focus and the usefulness of flexible bronchoscopy in hemoptysis
