Risk Factors for the Development and Progression of Atlantoaxial Subluxation in Surgically Treated Rheumatoid Arthritis Patients, Considering the Time Interval between Rheumatoid Arthritis Diagnosis and Surgery
- Affiliations
-
- 1Department of Neurosurgery, Hanyang University Medical Center, Seoul, Korea. tdy815@hanyang.ac.kr
- 2Department of Neurosurgery, Hanyang University Guri Hospital, Guri, Korea.
- KMID: 2417341
- DOI: http://doi.org/10.3340/jkns.2016.59.6.590
Abstract
OBJECTIVE
Rheumatoid arthritis (RA) is a systemic disease that can affect the cervical spine, especially the atlantoaxial region. The present study evaluated the risk factors for atlantoaxial subluxation (AAS) development and progression in patients who have undergone surgical treatment.
METHODS
We retrospectively analyzed the data of 62 patients with RA and surgically treated AAS between 2002 and 2015. Additionally, we identified 62 patients as controls using propensity score matching of sex and age among 12667 RA patients from a rheumatology registry between 2007 and 2015. We extracted patient data, including sex, age at diagnosis, age at surgery, disease duration, radiographic hand joint changes, and history of methotrexate use, and laboratory data, including presence of rheumatoid factor and the C-reactive protein (CRP) level.
RESULTS
The mean patient age at diagnosis was 38.0 years. The mean time interval between RA diagnosis and AAS surgery was 13.6±7.0 years. The risk factors for surgically treated AAS development were the serum CRP level (p=0.005) and radiographic hand joint erosion (p=0.009). The risk factors for AAS progression were a short time interval between RA diagnosis and radiographic hand joint erosion (p<0.001) and young age at RA diagnosis (p=0.04).
CONCLUSION
The CRP level at RA diagnosis and a short time interval between RA diagnosis and radiographic hand joint erosion might be risk factors for surgically treated AAS development in RA patients. Additionally, a short time interval between RA diagnosis and radiographic hand joint erosion and young age at RA diagnosis might be risk factors for AAS progression.
MeSH Terms
Figure
-

Fig. 1 The number of surgically treated patients stratified into 6 categories based on a 5-year time interval between RA diagnosis and AAS surgery. A total of 53 (85.4%) patients underwent surgical treatment less than 20 years after RA diagnosis. RA : rheumatoid arthritis, AAS : atlantoaxial subluxation.
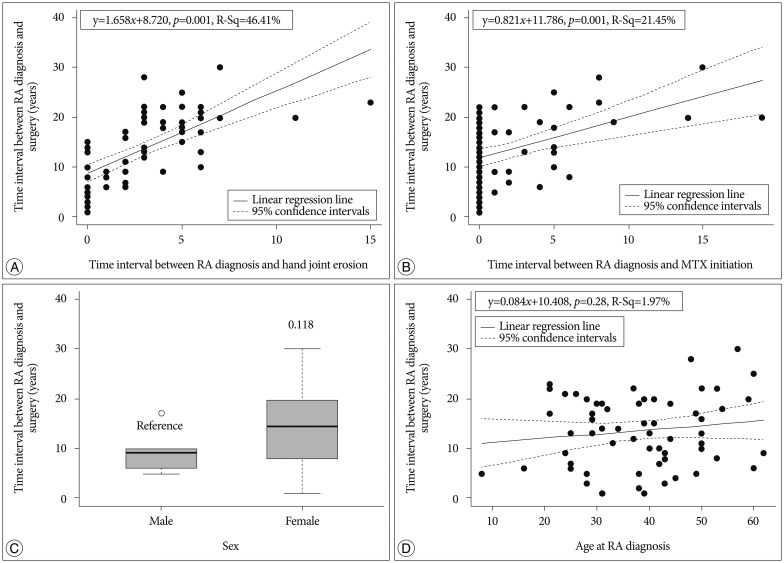
Fig. 2 A : In scatterplot graph, the linear regression line shows a statistically significant overall gradual upward slope, which means the time to surgery reduces by 1.658 years when the time to radiographic hand joint erosion reduces by 1 year. B : In scatterplot graph, the linear regression line shows a statistically significant overall gradual upward slope, indicating that patients who started MTX early required early surgery. C : The boxplot graph shows the mean time interval between RA diagnosis and AAS surgery was 4.7 years greater in female patients than in male patients. D : In scatterplot graph, the linear regression line shows an upward trend, indicating that patients who are diagnosed with RA at a young age might require early AAS surgery. RA : rheumatoid arthritis, AAS : atlantoaxial subluxation.
Reference
-
1. Ahn JK, Hwang JW, Oh JM, Lee J, Lee YS, Jeon CH. Risk factors for development and progression of atlantoaxial subluxation in Korean patients with rheumatoid arthritis. Rheumatol Int. 2011; 31:1363–1368. PMID: 20422194.
Article2. Alamanos Y, Drosos AA. Epidemiology of adult rheumatoid arthritis. Autoimmun Rev. 2005; 4:130–136. PMID: 15823498.
Article3. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988; 31:315–324. PMID: 3358796.
Article4. Blom M, Creemers MC, Kievit W, Lemmens JA, van Riel PL. Long-term follow-up of the cervical spine with conventional radiographs in patients with rheumatoid arthritis. Scand J Rheumatol. 2013; 42:281–288. PMID: 23311707.
Article5. Casey AT, Crockard HA, Bland JM, Stevens J, Moskovich R, Ransford AO. Surgery on the rheumatoid cervical spine for the non-ambulant myelopathic patient-too much, too late? Lancet. 1996; 347:1004–1007. PMID: 8606562.
Article6. Delamarter RB, Bohlman HH. Postmortem osseous and neuropathologic analysis of the rheumatoid cervical spine. Spine (Phila Pa 1976). 1994; 19:2267–2274. PMID: 7846570.
Article7. Fujiwara K, Fujimoto M, Owaki H, Kono J, Nakase T, Yonenobu K, et al. Cervical lesions related to the systemic progression in rheumatoid arthritis. Spine (Phila Pa 1976). 1998; 23:2052–2056. PMID: 9794048.
Article8. Hirano K, Imagama S, Oishi Y, Kanayama Y, Ito Z, Wakao N, et al. Progression of cervical instabilities in patients with rheumatoid arthritis 5.7 years after their first lower limb arthroplasty. Mod Rheumatol. 2012; 22:743–749. PMID: 22245951.
Article9. Ito H, Neo M, Sakamoto T, Fujibayashi S, Yoshitomi H, Nakamura T. Subaxial subluxation after atlantoaxial transarticular screw fixation in rheumatoid patients. Eur Spine J. 2009; 18:869–876. PMID: 19337758.
Article10. Joaquim AF, Appenzeller S. Cervical spine involvement in rheumatoid arthritis--a systematic review. Autoimmun Rev. 2014; 13:1195–1202. PMID: 25151973.11. Kaito T, Hosono N, Ohshima S, Ohwaki H, Takenaka S, Fujiwara H, et al. Effect of biological agents on cervical spine lesions in rheumatoid arthritis. Spine (Phila Pa 1976). 2012; 37:1742–1746. PMID: 22472805.
Article12. Konttinen YT, Bergroth V, Santavirta S, Sandelin J. Inflammatory involvement of cervical spine ligaments in patients with rheumatoid arthritis and atlantoaxial subluxation. J Rheumatol. 1987; 14:531–534. PMID: 3498036.13. Mathews JA. Atlanto-axial subluxation in rheumatoid arthritis. A 5-year follow-up study. Ann Rheum Dis. 1974; 33:526–531. PMID: 4441130.
Article14. Naranjo A, Carmona L, Gavrila D, Balsa A, Belmonte MA, Tena X, et al. Prevalence and associated factors of anterior atlantoaxial luxation in a nation-wide sample of rheumatoid arthritis patients. Clin Exp Rheumatol. 2004; 22:427–432. PMID: 15301239.15. Oda T, Fujiwara K, Yonenobu K, Azuma B, Ochi T. Natural course of cervical spine lesions in rheumatoid arthritis. Spine (Phila Pa 1976). 1995; 20:1128–1135. PMID: 7638655.
Article16. Ranawat CS, O'Leary P, Pellicci P, Tsairis P, Marchisello P, Dorr L. Cervical spine fusion in rheumatoid arthritis. J Bone Joint Surg Am. 1979; 61:1003–1010. PMID: 489640.
Article17. Raskin RJ, Schnapf DJ, Wolf CR, Killian PJ, Lawless OJ. Computerized tomography in evaluation of atlantoaxial subluxation in rheumatoid arthritis. J Rheumatol. 1983; 10:33–41. PMID: 6842484.18. Reiter MF, Boden SD. Inflammatory disorders of the cervical spine. Spine (Phila Pa 1976). 1998; 23:2755–2766. PMID: 9879101.
Article19. Renna R, Plantone F, Plantone D. Atlantoaxial subluxation in rheumatoid arthritis. J Rheumatol. 2013; 40:1925. PMID: 24187159.
Article20. Sharp J, Purser DW. Spontaneous atlanto-axial dislocation in ankylosing spondylitis and rheumatoid arthritis. Ann Rheum Dis. 1961; 20:47–77. PMID: 18623858.
Article21. van Asselt KM, Lems WF, Bongartz EB, Hamburger HL, Drossaers-Bakker KW, Dijkmans BA, et al. Outcome of cervical spine surgery in patients with rheumatoid arthritis. Ann Rheum Dis. 2001; 60:448–452. PMID: 11302865.
Article22. van der Heijde DM, van't Hof MA, van Riel PL, van Leeuwen MA, van Rijswijk MH, van de Putte LB. Validity of single variables and composite indices for measuring disease activity in rheumatoid arthritis. Ann Rheum Dis. 1992; 51:177–181. PMID: 1550400.
Article23. Winfield J, Cooke D, Brook AS, Corbett M. A prospective study of the radiological changes in the cervical spine in early rheumatoid disease. Ann Rheum Dis. 1981; 40:109–114. PMID: 7224682.
Article24. Yurube T, Sumi M, Nishida K, Miyamoto H, Kohyama K, Matsubara T, et al. Accelerated development of cervical spine instabilities in rheumatoid arthritis : a prospective minimum 5-year cohort study. PLoS One. 2014; 9:e88970. PMID: 24558457.25. Yurube T, Sumi M, Nishida K, Miyamoto H, Kohyama K, Matsubara T, et al. Incidence and aggravation of cervical spine instabilities in rheumatoid arthritis : a prospective minimum 5-year follow-up study of patients initially without cervical involvement. Spine (Phila Pa 1976). 2012; 37:2136–2144. PMID: 22895480.
Article26. Zhang T, Pope J. Cervical spine involvement in rheumatoid arthritis over time : results from a meta-analysis. Arthritis Res Ther. 2015; 17:148. PMID: 26026719.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rheumatoid Atlantoaxial Subluxation: Report of a Case
- A Case of Rheumatoid Arthritis Presenting Initially as Atlantoaxial Subluxation
- Surgical Management of Atlantoaxial Instability Due to Rheumatoid Arthritis
- Cytokines in rheumatoid arthritis
- Clinical significance of rheumatoid factor in juvenile rheumatoid arthritis
