Electrolyte Blood Press.
2018 Jun;16(1):15-17. 10.5049/EBP.2018.16.1.15.
Interstitial Nephritis Caused by Anorexia Nervosa in Young Male; A Case Report and Literature Review
- Affiliations
-
- 1Department of Internal Medicine, Chungbuk National University Hospital, Chungbuk National University College of Medicine, Cheongju, Korea. kwon@chungbuk.ac.kr
- 2Department of Pathology, Chungbuk National University Hospital, Chungbuk National University College of Medicine, Cheongju, Korea.
- KMID: 2416375
- DOI: http://doi.org/10.5049/EBP.2018.16.1.15
Abstract
- Severe eating disorders characterized by repetitive episodes of purging and vomiting can occasionally trigger acute kidney injury. However, interstitial nephritis induced by episodes of repeated vomiting has rarely been reported, and the pathophysiology of this entity remains unknown. A 26-year-old man was admitted to our hospital because of known hypokalemia. His serum electrolyte profile showed: sodium 133 mEq/L, potassium 2.6 mEq/L, chloride 72 mEq/L, total carbon dioxide 50 mEq/L, blood urea nitrogen/creatinine ratio (BUN/Cr) 21.9/1.98 mg/dL, and magnesium 2.0 mg/dL. Arterial blood gas analysis showed: pH 7.557, partial pressure of carbon dioxide 65.8 mmHg, and bicarbonate 58.5 mEq/L. His urinary potassium concentration was 73.2 mEq/L, and Cr was 111 mg/dL. Renal biopsy revealed acute tubular necrosis and tubulointerstitial nephritis with a few shrunken glomeruli. Repeated psychogenic vomiting may precipitate acute kidney injury and interstitial nephritis secondary to volume depletion and hypokalemia. Serum electrolyte levels and renal function should be carefully monitored in patients diagnosed with eating disorders to prevent tubular ischemia and interstitial nephritis.
MeSH Terms
Figure
-
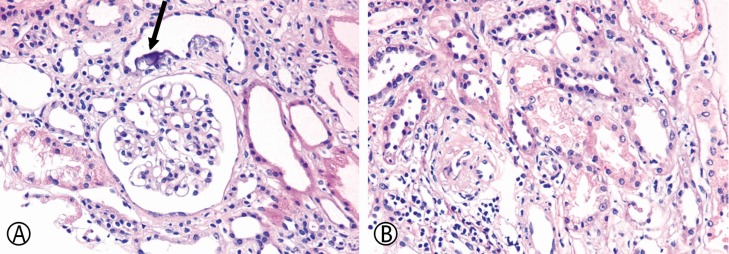
Fig. 1 (A) Renal tubules showing calcification below the epithelial cells (arrow) without definite glomerular abnormality (hematoxylin and eosin, ×400). (B) Vacuolar changes in the cytoplasm of cells of the proximal tubular epithelium. Mild nuclear variation, implying regeneration after acute damage, is also apparent (hematoxylin and eosin, ×400).
Reference
-
1. Hudson JI, Hiripi E, Pope HG, Kessler RC. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biol Psychiatry. 2007; 61:348–358. PMID: 16815322.
Article2. Luthra M, Davids MR, Shafiee MA, Halperin ML. Anorexia nervosa and chronic renal insufficiency: a prescription for disaster. QJM. 2004; 97:167–178. PMID: 14976274.
Article4. Li Cavoli G, Mulè G, Rotolo U. Renal involvement in psychological eating disorders. Nephron Clin Pract. 2011; 119:c338–c341. discussion c341. PMID: 22135793.
Article5. Ohashi N, Minemura S, Togawa A, Ohyama K. A case of hypokalemia-induced fatal arrhythmia caused by indapamide in an anorexic elderly patient. Clin Exp Nephrol. 2011; 15:761–764. PMID: 21671161.
Article6. Brotman AW, Stern TA, Brotman DL. Renal disease and dysfunction in two patients with anorexia nervosa. J Clin Psychiatry. 1986; 47:433–434. PMID: 3733679.7. Abdel-Rahman EM, Moorthy AV. End-stage renal disease (ESRD) in patients with eating disorders. Clin Nephrol. 1997; 47:106–111. PMID: 9049458.8. Sim LA, McAlpine DE, Grothe KB, Himes SM, Cockerill RG, Clark MM. Identification and treatment of eating disorders in the primary care setting. Mayo Clin Proc. 2010; 85:746–751. PMID: 20605951.
Article9. Riemenschneider T, Bohle A. Morphologic aspects of lowpotassium and low-sodium nephropathy. Clin Nephrol. 1983; 19:271–279. PMID: 6872364.10. Arimura Y, Tanaka H, Yoshida T, Shinozaki M, Yanagida T, Ando T, et al. Anorexia nervosa: an important cause of chronic tubulointerstitial nephropathy. Nephrol Dial Transplant. 1999; 14:957–959. PMID: 10328479.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pericardial effusion in three cases of anorexia nervosa
- Successful Treatment of Anorexia Nervosa in a 10-year-old Boy with Risperidone Long-acting Injection
- A Case of Acute Gastric Dilatation with Duodenal Obstruction Accompanying Elevated Serum Pancreatic Enzymes in a Patient with Bulimia
- Anorexia Nervosa with Autonomic Dysfunction
- A Case of Anorexia Nervosa with Gelatinous Transformation of Marrow
