J Clin Neurol.
2018 Jul;14(3):407-412. 10.3988/jcn.2018.14.3.407.
Mechanical Thrombectomy in Strokes with Large-Vessel Occlusion Beyond 6 Hours: A Pooled Analysis of Randomized Trials
- Affiliations
-
- 1Department of Neurology and Stroke Unit, Sant'Anna Hospital, Como, Italy. simone.vidale@asst-lariana.it
- 2Department of Neurology and Stroke Unit, Niguarda Ca' Granda Hospital, Milan, Italy.
- 3Department of Neuroradiology, San Gerardo Hospital, Monza, Italy.
- KMID: 2415060
- DOI: http://doi.org/10.3988/jcn.2018.14.3.407
Abstract
- BACKGROUND AND PURPOSE
Mechanical thrombectomy with or without intravenous thrombolysis is indicated in the acute treatment of ischemic strokes caused by an emergent large-vessel occlusion (ELVO) within 6 hours from symptom onset. However, a significant proportion of patients are referred to comprehensive stroke centers beyond this therapeutic time window. This study performed a pooled analysis of data from trials in which mechanical thrombectomy was performed beyond 6 hours from symptom onset.
METHODS
We searched for randomized controlled trials that compared mechanical thrombectomy with the best medical treatment beyond 6 hours for ischemic strokes due to ELVO and reported on between 1990 and April 2018. The intervention group comprised patients treated with mechanical thrombectomy. Statistical analysis was conducted while pooling data and analyzing fixed- or random-effects models as appropriate.
RESULTS
Four trials involving 518 stroke patients met the eligibility criteria. There were 267 strokes treated with mechanical thrombectomy, with a median time of 10.8 hours between when the patient was last known to be well to randomization. We observed a significant difference between groups concerning the rate of functional independence at 90 days from stroke, with an absolute difference of 27.5% (odds ratio=3.33, 95% CI=1.81-6.12, p < 0.001) and good recanalization (odds ratio=13.17, 95% CI=4.17-41.60, p < 0.001) favoring the intervention group.
CONCLUSIONS
This meta-analysis confirms the efficacy of mechanical thrombectomy in selected ischemic stroke patients beyond 6 hours from symptom onset. The selection is mainly based on the limited core infarct detected by emergent assessment using neuroimaging techniques.
Keyword
Figure
-
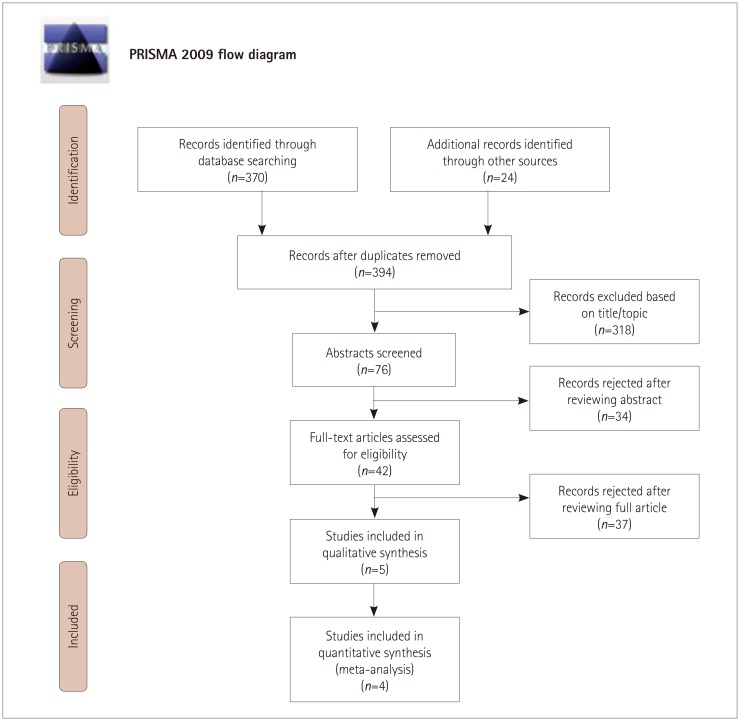
Fig. 1 PRISMA flow diagram. Adapted from Moher et al.9 Plos Med 2009;6:e1000097.

Fig. 2 Forest plot of the primary endpoint.
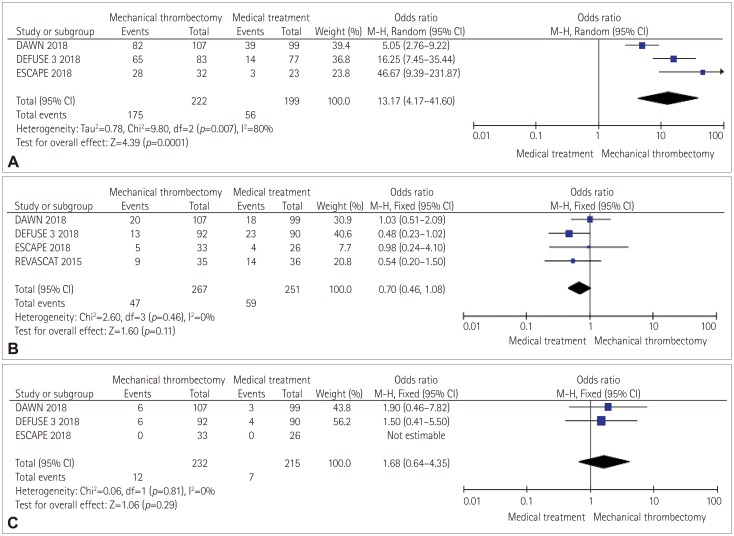
Fig. 3 Forest plots of the secondary endpoints: (A) good recanalization, (B) death at 90 days after stroke, and (C) symptomatic intracranial hemorrhage.
Cited by 1 articles
-
Pull-Through Buddy Wire Technique for Endovascular Thrombectomy in Patients with Acute Ischemic Stroke: Technical Note
Pin-Yi Chiang, Yen-Heng Lin, Yu-Cheng Huang, Chung-Wei Lee
Neurointervention. 2021;16(1):64-69. doi: 10.5469/neuroint.2020.00409.
Reference
-
1. Saver JL, Goyal M, van der Lugt A, Menon BK, Majoie CB, Dippel DW, et al. Time to treatment with endovascular thrombectomy and outcomes from ischemic stroke: a meta-analysis. JAMA. 2016; 316:1279–1288. PMID: 27673305.
Article2. Smith EE, Saver JL, Cox M, Liang L, Matsouaka R, Xian Y, et al. Increase in endovascular therapy in Get With The Guidelines-Stroke after the publication of the pivotal trials. Circulation. 2017; 136:2303–2310. PMID: 28982689.3. Bang OY, Goyal M, Liebeskind DS. Collateral circulation in ischemic stroke: assessment tools and therapeutic strategies. Stroke. 2015; 46:3302–3309. PMID: 26451027.4. Albers GW, Marks MP, Kemp S, Christensen S, Tsai JP, Ortega-Gutierrez S, et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med. 2018; 378:708–718. PMID: 29364767.
Article5. Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 2018; 378:11–21. PMID: 29129157.6. Hacke W, Kaste M, Fieschi C, von Kummer R, Davalos A, Meier D, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet. 1998; 352:1245–1251. PMID: 9788453.7. Evans JW, Graham BR, Pordeli P, Al-Ajlan FS, Willinsky R, Montanera WJ, et al. Time for a time window extension: insights from late presenters in the ESCAPE trial. AJNR Am J Neuroradiol. 2018; 39:102–106. PMID: 29191873.
Article8. Jovin TG, Chamorro A, Cobo E, de Miquel MA, Molina CA, Rovira A, et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med. 2015; 372:2296–2306. PMID: 25882510.
Article9. Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009; 6:e1000097. PMID: 19621072.
Article10. Kamal N, Majmundar N, Damadora N, El-Ghanem M, Nuoman R, Keller IA, et al. Mechanical thrombectomy-is time still brain? The DAWN of a new era. Br J Neurosurg. 2018; 2. 08. DOI: 10.1080/02688697.2018.1426726. [Epub].11. Sheth SA, Sanossian N, Hao Q, Starkman S, Ali LK, Kim D, et al. Collateral flow as causative of good outcomes in endovascular stroke therapy. J Neurointerv Surg. 2016; 8:2–7. PMID: 25378639.
Article12. Liebeskind DS, Tomsick TA, Foster LD, Yeatts SD, Carrozzella J, Demchuk AM, et al. Collaterals at angiography and outcomes in the Interventional Management of Stroke (IMS) III trial. Stroke. 2014; 45:759–764. PMID: 24473178.
Article13. Telischak NA, Wintermark M. Imaging predictors of procedural and clinical outcome in endovascular acute stroke therapy. Neurovasc Imaging. 2015; 1:4.
Article15. Wareham J, Phan K, Renowden S, Mortimer AM. A meta-analysis of observational evidence for the use of endovascular thrombectomy in proximal occlusive stroke beyond 6 hours in patients with limited core infarct. Neurointervention. 2017; 12:59–68. PMID: 28955507.
Article16. Badhiwala JH, Nassiri F, Alhazzani W, Selim MH, Farrokhyar F, Spears J, et al. Endovascular thrombectomy for acute ischemic stroke: a meta-analysis. JAMA. 2015; 314:1832–1843. PMID: 26529161.17. Vidale S, Agostoni E. Endovascular treatment of ischemic stroke: an updated meta-analysis of efficacy and safety. Vasc Endovascular Surg. 2017; 51:215–219. PMID: 28424039.
Article18. Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016; 387:1723–1731. PMID: 26898852.
Article19. Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018; 49:e46–e110. PMID: 29367334.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Emergency management of stroke in the era of mechanical thrombectomy
- Paradigm Shift in Intra-Arterial Mechanical Thrombectomy for Acute Ischemic Stroke : A Review of Randomized Controlled Trials after 2015
- Mechanical Thrombectomy for Large Vessel Occlusion via the Transbrachial Approach: Case Series
- Endovascular Treatment of Large Vessel Occlusion Strokes Due to Intracranial Atherosclerotic Disease
- Differences in mechanical thrombectomy for acute ischemic stroke on weekdays versus nights/ weekends in a Japanese primary stroke core center
