J Rhinol.
2018 May;25(1):51-54. 10.18787/jr.2018.25.1.51.
A Case of Congenital Defect of the Lateral Crus of the Lower Lateral Cartilage
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Institute of Wonkwang Medical Science, College of Medicine, Wonkwang University, Iksan, Korea. Leejaehoon64@gmail.com
- KMID: 2412922
- DOI: http://doi.org/10.18787/jr.2018.25.1.51
Abstract
- Congenital anomalies of the nose are distinctly unusual and appear at an incidence of 1 in 20,000 to 40,000 live births. Embrio-logically, developmental defects in the lateral nasal processes result in anomalies of the alar region. The defects of the lower lateral cartilage on one side and the different sizes of lower lateral cartilages cause problems in nasal tip support, contour, and symmetry. We present a case of congenital defect of the lateral crus of the right lower lateral cartilage of a 43-year-old male. The defect of the right lateral crus was reconstructed with the cartilage graft and the upper portion and the lateral crus of the left lower lateral cartilage were partially resected for symmetry of the nasal tip.
Keyword
Figure
-

Fig. 1 Frontal (A) and basal (B) views of the nose shows profound nasal tip and nostril asymmetry.

Fig. 2 A schematic picture of congenital total defect of the lateral crus of the right lower lateral cartilage.
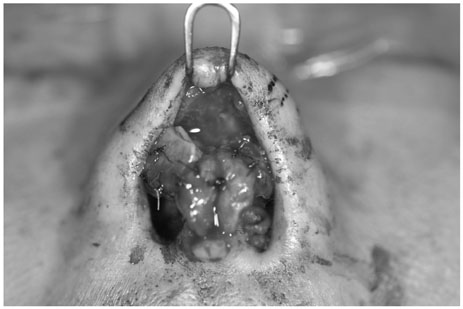
Fig. 3 At surgery, the total defect of the right lateral crus was found. The replacement graft (16×9×3.5 mm) on the defect area was done with septal cartilage. The upper portion and lateral crus of the left lower lateral cartilage were resected 3 mm, 4 mm, respectively.
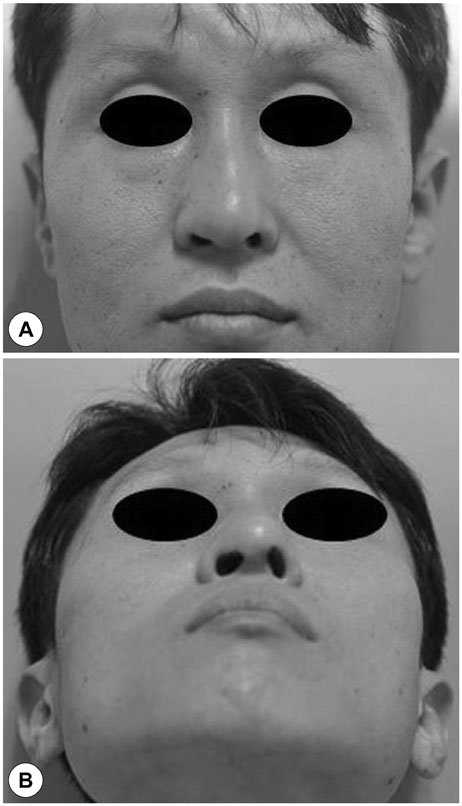
Fig. 4 Ten months after the rhinoplasty frontal (A) and basal (B) views of the nose show the aesthetic good results, despite of the persistence of nostril asymmetry.
Reference
-
1. Losee JE, Kirschner RE, Whitaker LA, Bartlett SP. Congenital nasal anomalies: a classification scheme. Plast Reconstr Surg. 2004; 113(2):676–689.
Article2. Adelson RT, Karimi K, Herrero N. Isolated congenital absence of the left lower lateral cartilage. Otolaryngol Head Neck Surg. 2008; 138(6):793–794.
Article3. Kosins AM, Daniel RK, Sajjadian A, Helms J. Rhinoplasty: congenital deficiencies of the alar cartilage. Aesthet Surg J. 2013; 33(6):799–808.4. Temiz G, Yeşiloğlu N, Sarici M, Filinte GT. Congenital isolated aplasia of lower lateral cartilage and reconstruction using dorsal hump material. J Craniofac Surg. 2014; 25(5):e411–e413.
Article5. Carlson BM. Development of head and neck. Human embryology and developmental biology. St Louis: Mosby;1994. p. 283–286.6. Couly G. Neurocristopathies of the Neurocristopathies of the human nasofrontal bud: ethmoidal syndromes (hypo- and hyper-septoethmoidism). Rev Stomatol Chir Maxillofac. 1981; 82(4):213–225.7. Gitton Y, Benouaiche L, Vincent C, Heude E, Soulika M, Bouhali K, et al. Dlx5 and Dlx6 expression in the anterior neural fold is essential for patterning the dorsal nasal capsule. Development. 2011; 138(5):897–903.
Article8. Cordero D, Marcucio R, Hu D, Gaffield W, Tapadia M, Helms JA. Temporal perturbations in sonic hedgehog signaling elicit the spectrum of holoprosencephaly phenotypes. J Clin Invest. 2004; 114(4):485–494.
Article9. Daniel RK. The nasal tip: anatomy and aesthetics. Plast Reconstr Surg. 1992; 89(2):216–224.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- New Anatomical Point of View of Alar Cartilage in Cleft Lip Nose Deformity and the Effects of Removal of Intercartilagenous Soft Tissue on Relocaton of Alar Cartilage
- Medial and Lateral Crus Elevation to Correct the Secondary Unilateral Cleft Lip-Nasal Deformities
- Effects of Release of Tip Supporting Fibrous Tissues for Short Nose Correction
- An Anthropometric Study of Lateral Crus of Alar Cartilages in Koreans
- Correction of Alar Cartilage Malposition
