Spectrum of Multi-Detector Computed Tomography Findings that Alter Pulmonary Artery Diameters in Adults
- Affiliations
-
- 1Department of Radiology, Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea. ytokim@schmc.ac.kr
- KMID: 2412357
- DOI: http://doi.org/10.3348/jksr.2018.78.6.389
Abstract
- Abnormalities in the anatomy of pulmonary arteries may have heritable or environmental causes and involve a reduction or enlargement in transverse diameters of the blood vessels eg, congenital and developmental disorders, acquired intrinsic causes, extrinsic compression, and constriction. Pulmonary hypertension, pulmonary artery aneurysm and pseudoaneurysm, and idiopathic dilatation can also increase the diameter of a pulmonary artery. Multi-detector computed tomography (CT) is useful to evaluate each pulmonary artery and to diagnose the conditions that alter the diameter of the pulmonary artery. It is important to be familiar with the CT features of a variety of disorders to allow for accurate diagnoses and appropriate therapeutic management.
MeSH Terms
Figure
-

Fig. 1. Interruption of the right pulmonary artery in an 18-year-old man. A. Axial images show a complete absence of the right main pulmonary artery, a small right lung, and mediastinal shifting to the right side. B. Axial image with lung window settings shows a small right lung with irregular linear opacities (arrowheads) in the lung periphery. C. On angiography of the right internal thoracic artery, left (arrow) and right (open arrow) portions of the right lung are supplied by the right internal thoracic artery. These systemic collaterals are shown as reticular opacities in the periphery of the affected lung on computed tomography.

Fig. 2. Constriction of the right pulmonary artery in an 85-year-old woman. Axial and coronal images show focal narrowing of the upper wall of the proximal right pulmonary artery (open arrowheads). The cause of pulmonary artery stenosis is thought to be idiopathic because there is no evidence of arterial wall thickening or surrounding soft tissue mass.

Fig. 3. Hypoplastic left pulmonary artery associated with lobar agenesis of the lung in a 40-year-old woman. Serial axial images with a mediastinal setting (A) show an anomalous hypoplastic left pulmonary artery. On the axial image with a lung window setting and coronal reformatted image (B), the normal positioned right upper lobe bronchus is absent, and the right major fissure is displaced anteriorly (arrows). Also, the bifurcation of the left main bronchus is not seen, and the hypoplastic left lung consists of a single lobe.
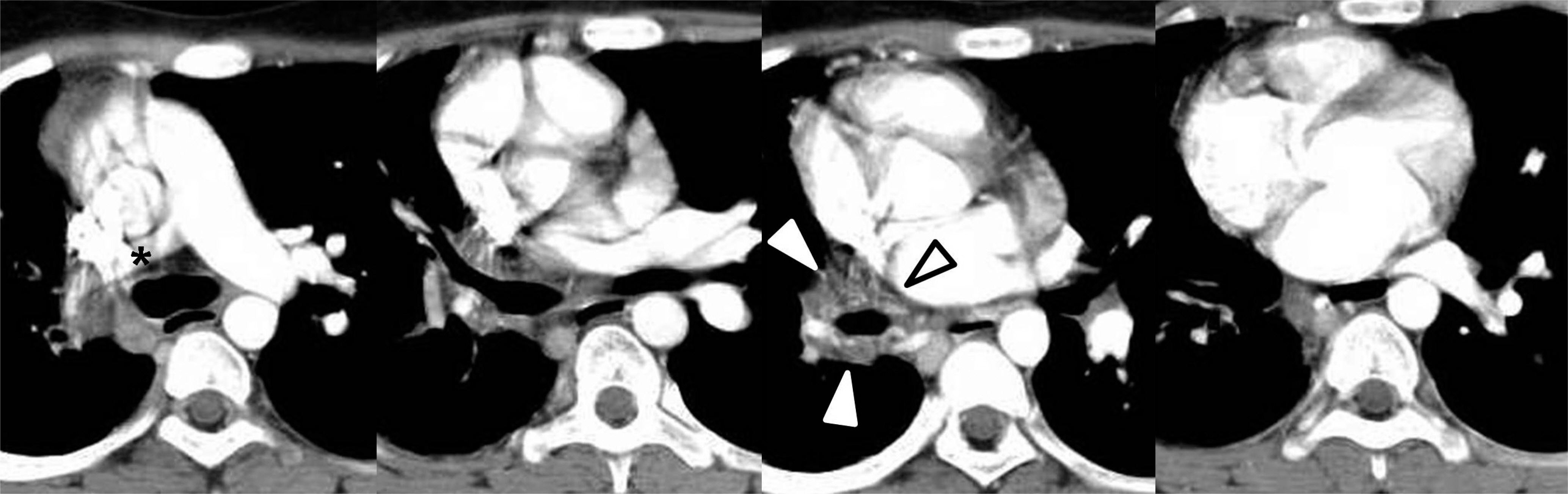
Fig. 4. Hypoplastic right pulmonary artery associated with right pulmonary vein atresia in a 14-year-old teenage girl. Serial axial images show a smooth left atrial margin (black open arrowhead) and absent right superior and inferior pulmonary veins. The adjacent soft tissue opacity (arrowheads) around the left atrium suggests collaterals. The right pulmonary artery (∗) is diffusely narrowed.

Fig. 5. Hypoplastic left pulmonary artery in Swyer-James syndrome in a 61-year-old man. A. Serial axial images showed a relatively small left pulmonary artery (∗) and decreased interlobar and segmental arteries (arrows) in the left lower lobe. B. Coronal image with lung window settings shows diffuse air trapping in the left lung with multifocal bronchiectasis and an irregularly shaped nodule in the left upper lobe. The volume of the left lung is not decreased. C. Anterior volume rendering image shows decreased pulmonary vascularity of the left lung.
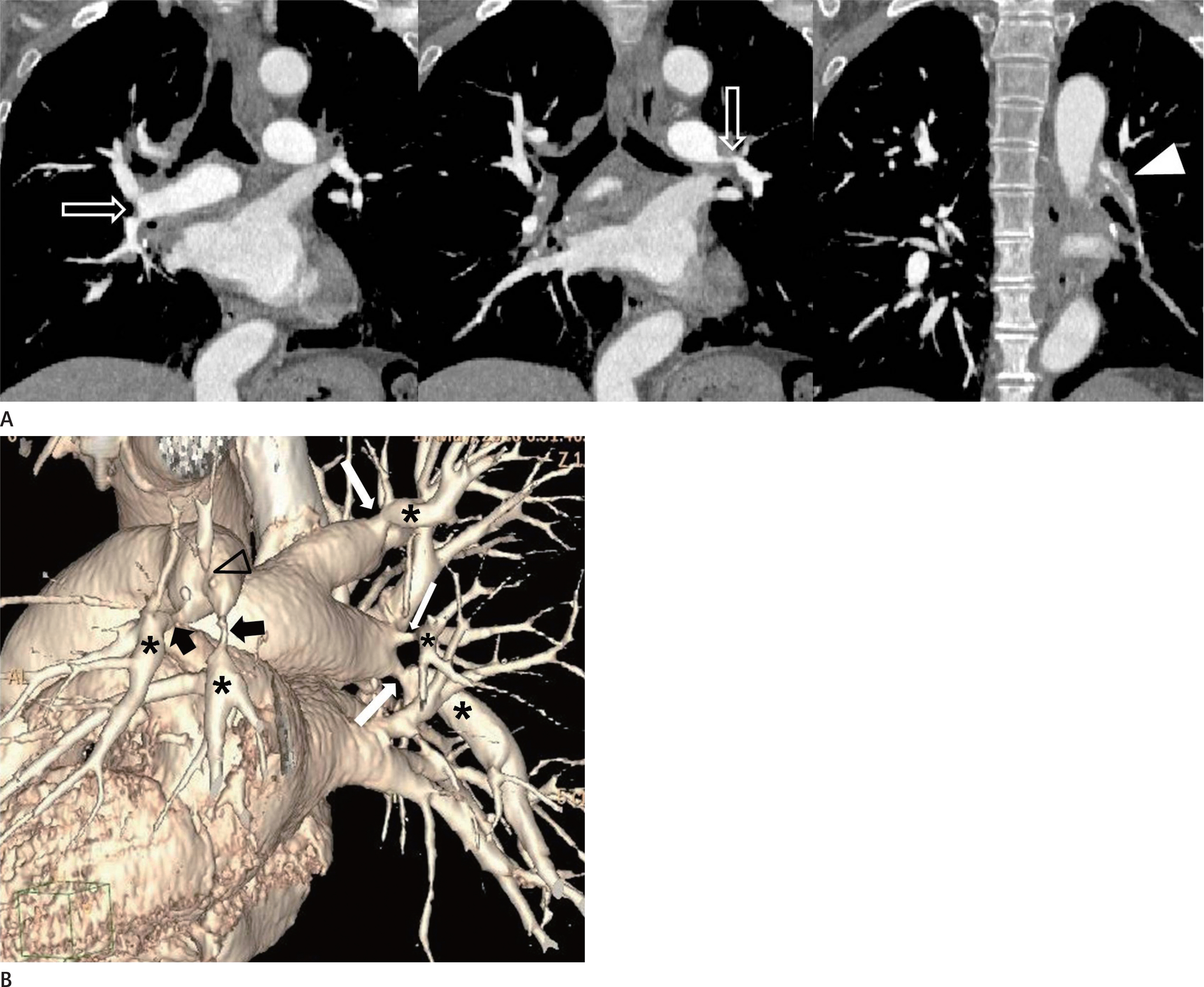
Fig. 6. Multiple stenoses and post-stenotic dilatation of the bilateral pulmonary arteries by chronic pulmonary thromboembolism in a 56-year-old man. A. Coronal images show narrowing bilateral pulmonary arteries at the bifurcation site (open arrows) and irregularly shaped intraluminal thrombi (arrowhead) in the inferior inter-lobar artery of the left lower lobe. B. The volume rendering three-dimensional image in left posterolateral projection showed multiple narrowing of the right (white arrows) and left (black arrows) pulmonary arteries with post-stenotic dilatation (∗). Also, note the discontinuity of the pulmonary artery (open black arrowhead) on the left upper lobe.

Fig. 7. Complete occlusion of the right pulmonary artery by chronic pulmonary thromboembolism in an 81-year-old man. Initial axial computed tomography image shows thromboembolism (∗) of the right pulmonary artery and follow-up axial image obtained eight years later indicates a complete occlusion in the mid-portion of the right pulmonary artery (arrow).

Fig. 8. Extrinsic compression of the right pulmonary artery by an aortic aneurysm in a 36-year-old man who was diagnosed with Marfan syndrome. Axial computed tomography image shows extrinsic compression of the main and right pulmonary arteries (∗) by an aneurysm in the ascending thoracic aorta.
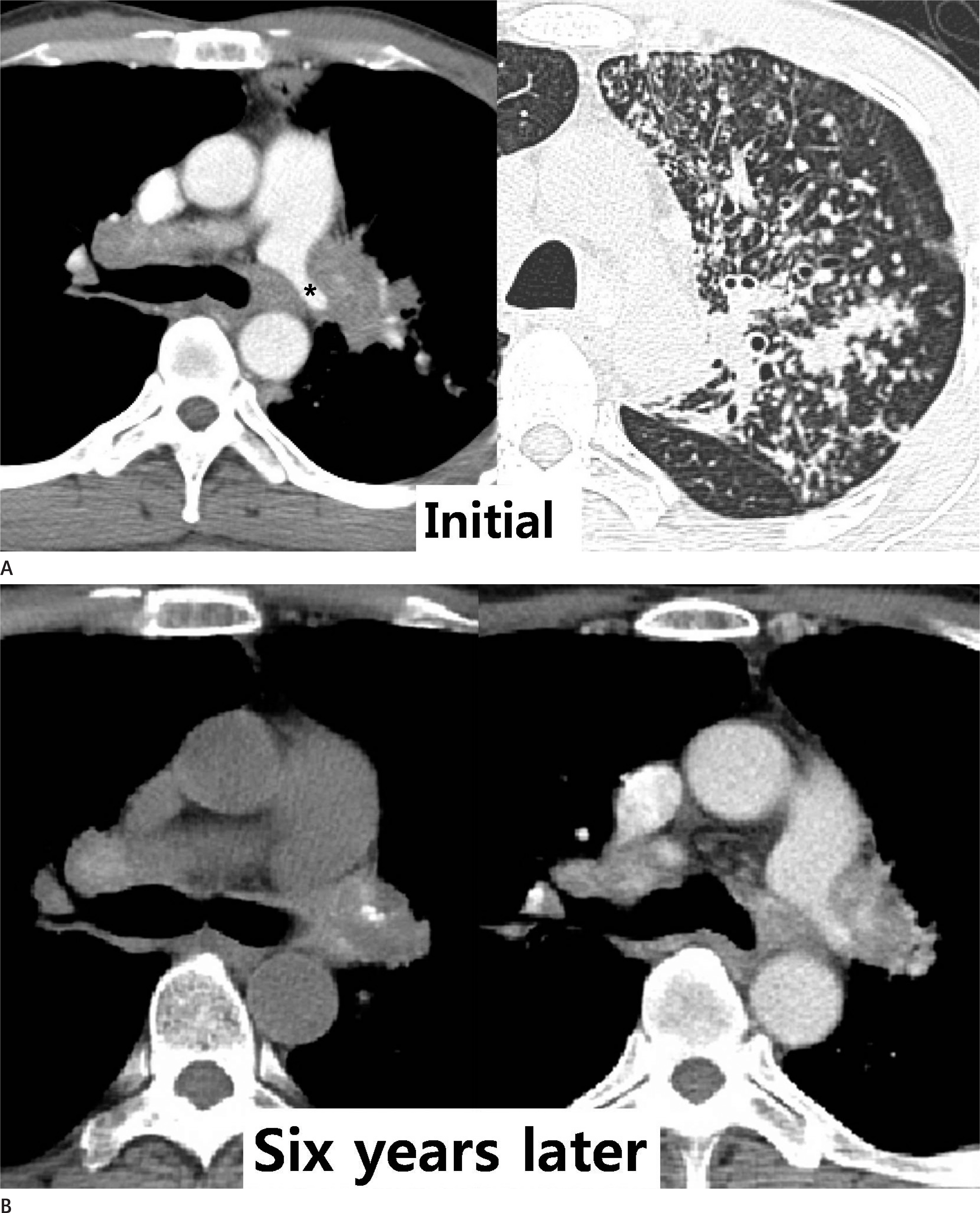
Fig. 9. Constriction of the left pulmonary artery by fibrosing mediastinitis in a 46-year-old woman. A. Initial axial images show an irregularly shaped mass-like lesion with a narrowing left pulmonary artery (∗) and axial image with lung window settings show active pulmonary tuberculosis in the left upper lobe. B. Axial images after six years show left pulmonary artery narrowing by a soft tissue mass that has focal calcification and diffuses high attenuation on unenhanced computed tomography. Despite improved active pulmonary tuberculosis in the left upper lobe, mediastinal fibrosis by tuberculosis has not changed.
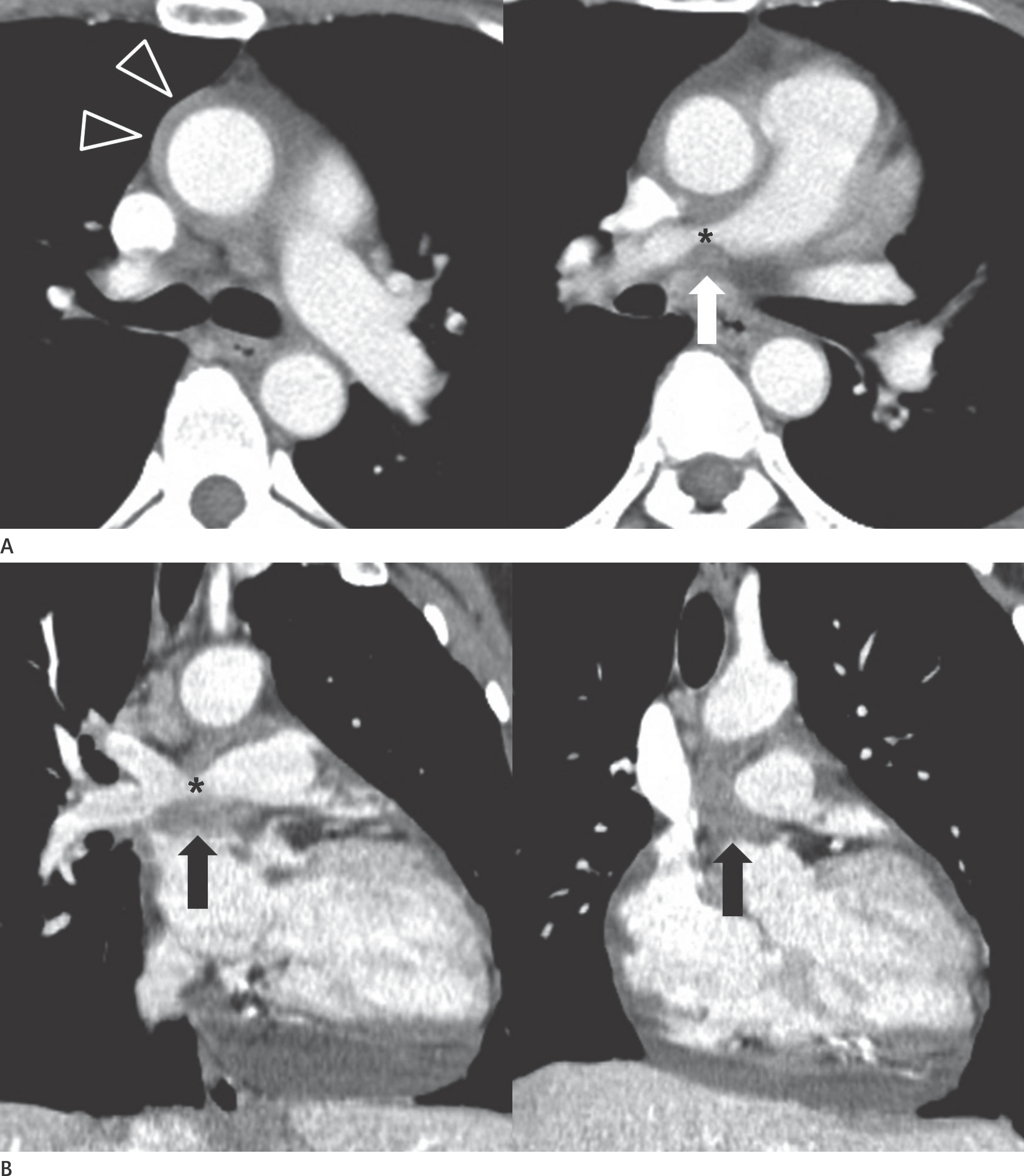
Fig. 10. Constriction of the right pulmonary artery by chronic pericarditis in a 47-year-old woman. A. Axial images show circumferential soft tissue attenuation (open arrowheads) around the ascending thoracic aorta and focal narrowing of the right pulmonary artery (∗) with surrounding soft tissue lesion (arrow). B. Coronal images show focal narrowing (∗) of the right pulmonary artery by a pericardial soft tissue mass (arrows); it was histologically confirmed as chronic inflammation of the pericardium by pericardiotomy.
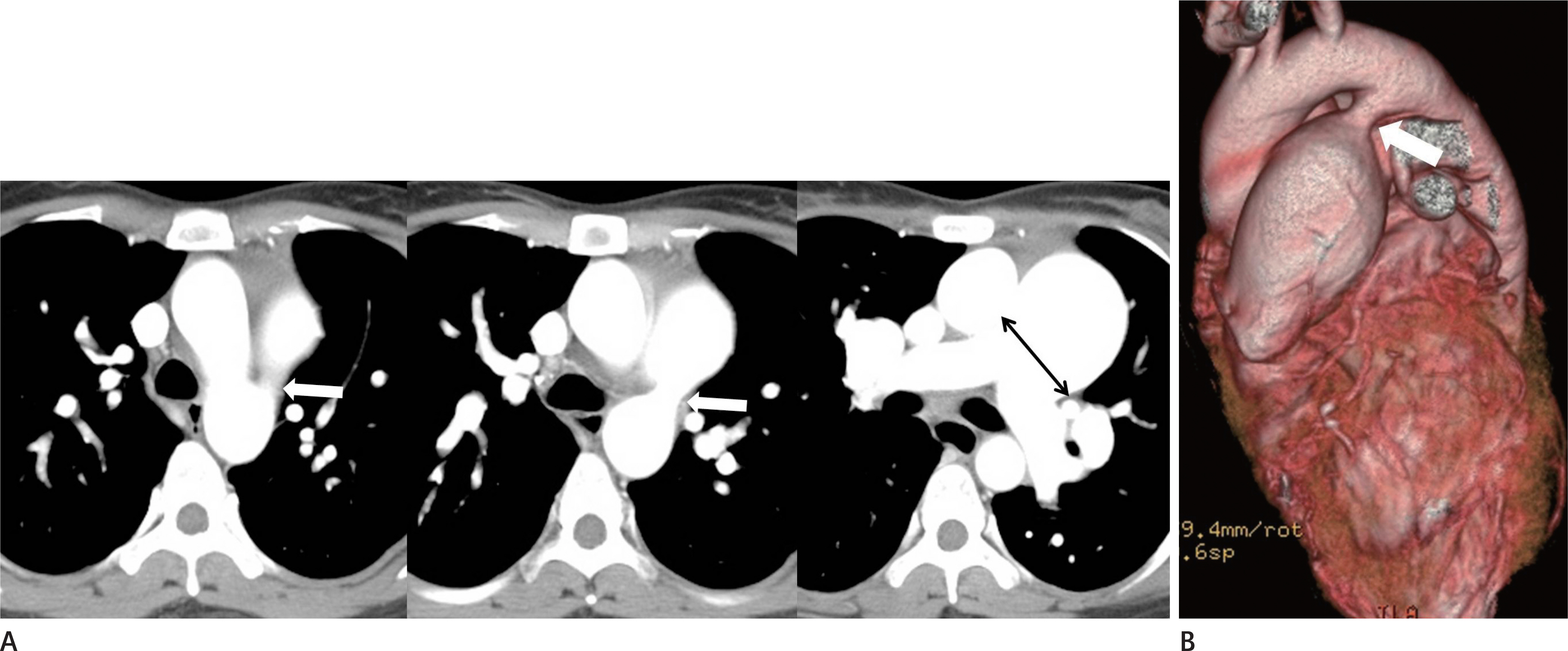
Fig. 11. Pulmonary hypertension secondary to patent ductus arteriosus in a 28-year-old woman. A, B. Serial axial images (A) show a main pulmonary artery dilated to more than 29 mm. There is direct communication (arrows) between the main pulmonary artery and the descending thoracic aorta on axial (A) and volume rendering images (B). The main pulmonary artery size is typically measured at the level of bifurcation of the main pulmonary artery perpendicular to the vessel wall (double-headed arrow). The upper limit of the normal main pulmonary artery diameter is 29 mm and that of the right interlobar artery is 17 mm on computed tomography.
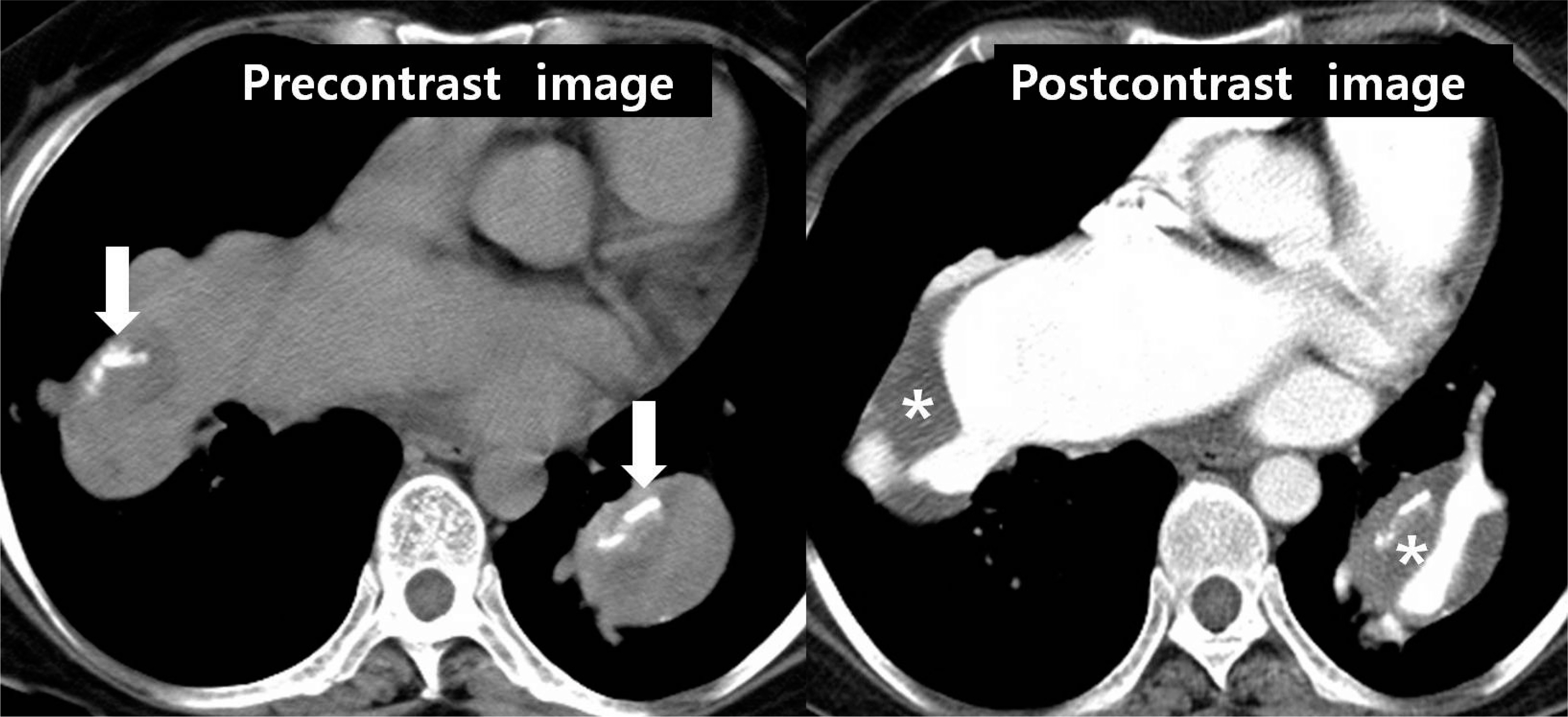
Fig. 12. Pulmonary hypertension in a 28-year-old woman who has been diagnosed with ASD. Post-contrast axial image shows that the diameters of the main and proximal lobar pulmonary arteries are increased secondary to ASD and thromboembolism (∗) in the dilated bilateral inter-lobar pulmonary arteries; eccentric calcifications (arrows) in the thrombi on pre-contrast image indicates chronic pulmonary thromboembolism. ASD = atrial septal defect

Fig. 13. Pulmonary pseudoaneurysm secondary to fungal infection in a 66-year-old man. A. Axial images show an aneurysmal sac (∗) within the necrotic portion of the diffuse consolidation in the left lung. B. Pulmonary angiography of the left lung shows an aneurysmal sac (∗) in the lingular segment. Bronchoscopic biopsy revealed fungal hyphae and was positive on both periodic acid-Schiff stain and Grocott methenamine silver stain. The sac was diagnosed as pseudoaneurysm by a fungal infection.
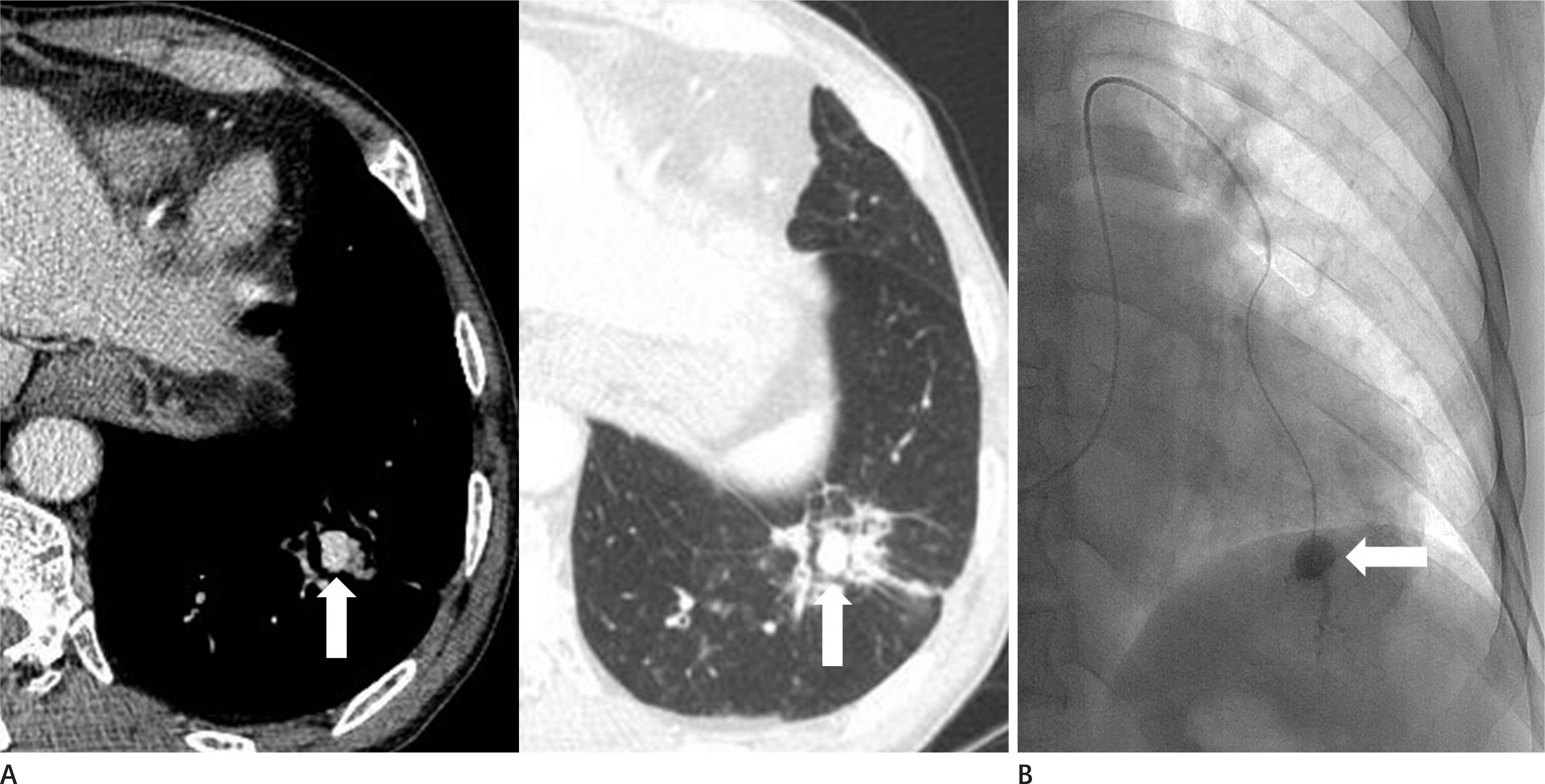
Fig. 14. Aneurysm of the peripheral pulmonary artery in a 66-year-old man who was treated 20 days earlier for pneumonia. A. Axial images show a highly enhanced aneurysm (arrows) and surrounding consolidation in the left lower lobe. B. Pulmonary angiography shows a small aneurysm (arrow) in the peripheral pulmonary artery in the left lower lobe. It was thought to be a pseudoaneurysm secondary to pneumonia.
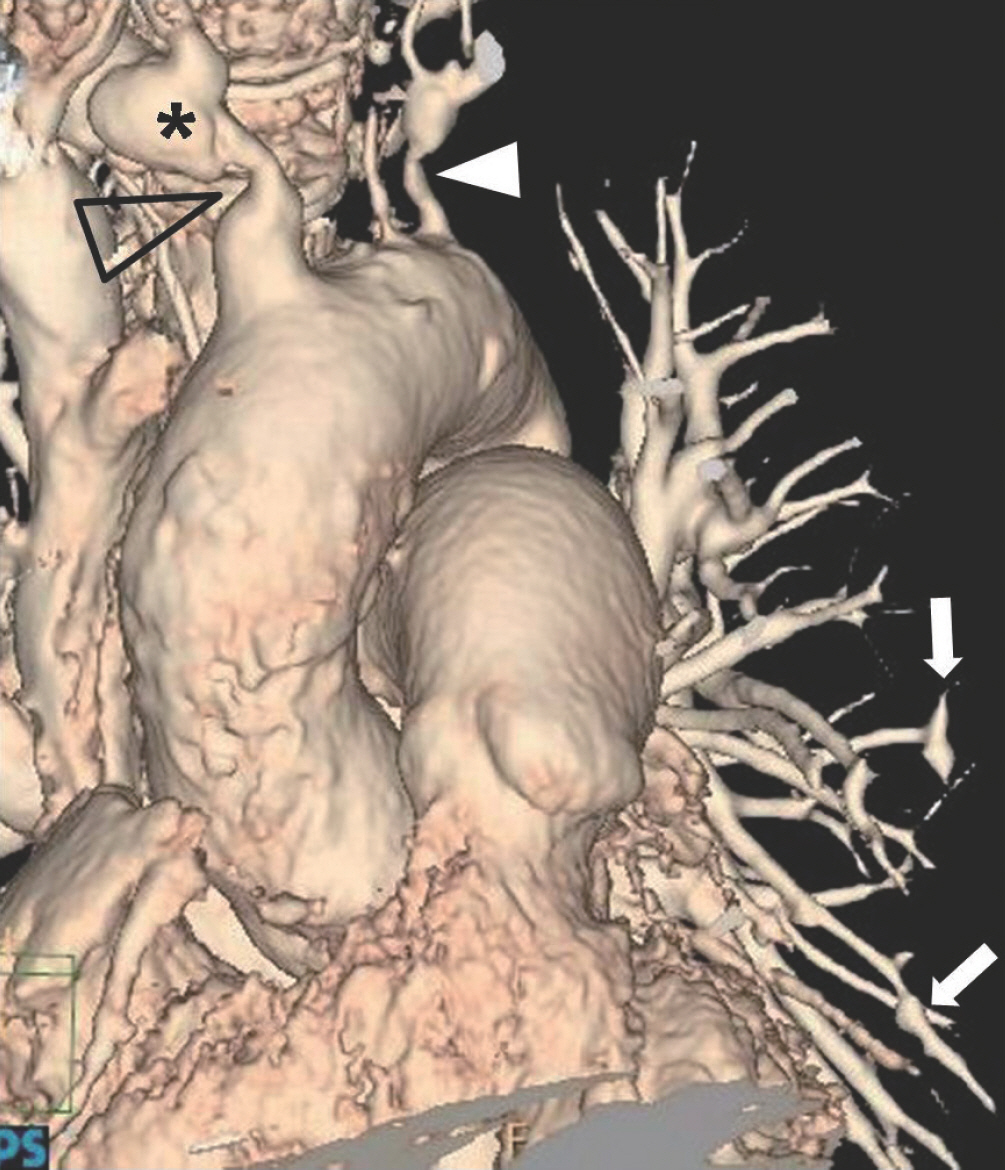
Fig. 15. Focal dilatation of the peripheral pulmonary arteries in a 54-year-old man who has been diagnosed with Takayasu arteritis. Anterior volume rendering computed tomography image shows focal dilatation of the peripheral pulmonary arteries (arrows) in the left lower lung. Also, note focal narrowing (open arrowhead) and poststenotic dilatation (∗) of the right brachiocephalic artery and stenosis (arrowhead) of the left subclavian artery.
Reference
-
References
1. Edwards PD, Bull RK, Coulden R. CT measurement of main pulmonary artery diameter. Br J Radiol. 1998; 71:1018–1020.
Article2. Kuriyama K, Gamsu G, Stern RG, Cann CE, Herfkens RJ, Brundage BH. CT-determined pulmonary artery diameters in predicting pulmonary hypertension. Invest Radiol. 1984; 19:16–22.
Article3. Truong QA, Massaro JM, Rogers IS, Mahabadi AA, Kriegel MF, Fox CS, et al. Reference values for normal pulmonary artery dimensions by noncontrast cardiac computed tomography: the Framingham Heart Study. Circ Cardiovasc Imaging. 2012; 5:147–154.4. Castañer E, Gallardo X, Rimola J, Pallardó Y, Mata JM, Per-endreu J, et al. Congenital and acquired pulmonary artery anomalies in the adult: radiologic overview. Radiographics. 2006; 26:349–371.
Article5. Schoepf UJ, Costello P. CT angiography for diagnosis of pulmonary embolism: state of the art. Radiology. 2004; 230:329–337.
Article6. Jones SE, Wittram C. The indeterminate CT pulmonary angiogram: imaging characteristics and patient clinical outcome. Radiology. 2005; 237:329–337.
Article7. Wittram C. How i do it: CT pulmonary angiography. AJR Am J Roentgenol. 2007; 188:1255–1261.
Article8. Mayo J, Thakur Y. Pulmonary CT angiography as first-line imaging for PE: image quality and radiation dose considerations. AJR Am J Roentgenol. 2013; 200:522–528.
Article9. Seymour J, Emanuel R, Pattinson N. Acquired pulmonary stenosis. Br Heart J. 1968; 30:776–785.
Article10. Do KH, Goo JM, Im JG, Kim KW, Chung JW, Park JH. Systemic arterial supply to the lungs in adults: spiral CT findings. Radiographics. 2001; 21:387–402.
Article11. Davies M, Guest PJ. Developmental abnormalities of the great vessels of the thorax and their embryological basis. Br J Radiol. 2003; 76:491–502.
Article12. Hislop A. Developmental biology of the pulmonary circulation. Paediatr Respir Rev. 2005; 6:35–43.
Article13. Anand SH, Jasper A, Mani SE, Joseph E, Mathai J. Proximal interruption of the pulmonary artery: a case series. J Clin Diagn Res. 2015; 9:TD04–TD06.
Article14. Ryu DS, Spirn PW, Trotman-Dickenson B, Hunsaker A, Jung SM, Park MS, et al. HRCT findings of proximal interruption of the right pulmonary artery. J Thorac Imaging. 2004; 19:171–175.
Article15. Choe YH, Ko JK, Lee HJ, Kang IS, Park PW, Lee YT. MR imaging of non-visualized pulmonary arteries at angiography in patients with congenital heart disease. J Korean Med Sci. 1998; 13:597–602.
Article16. Sondheimer HM, Oliphant M, Schneider B, Kavey RE, Blackman MS, Parker FB Jr. Computerized axial tomography of the chest for visualization of “absent” pulmonary arteries. Circulation. 1982; 65:1020–1025.
Article17. Franch RH, Gay BB Jr. Congenital stenosis of the pulmonary artery branches. a classification, with postmortem findings in two cases. Am J Med. 1963; 35:512–529.18. Baum D, Khoury GH, Ongley PA, Swan HJ, Kincaid OW. Congenital stenosis of the pulmonary artery branches. Circulation. 1964; 29:680–687.
Article19. Isawa T, Taplin GV. Unilateral pulmonary artery agenesis, stenosis, and hypoplasia. Radiology. 1971; 99:605–612.
Article20. Stovin PG. Early lung development. Thorax. 1985; 40:401–404.
Article21. Park S, Cha YK, Kim JS, Kwon JH, Jeong YJ, Kim SJ. Isolated unilateral pulmonary artery hypoplasia with accompanying pulmonary parenchymal findings on CT: a case report. J Korean Soc Radiol. 2017; 76:369–373.
Article22. Dixit R, Kumar J, Chowdhury V, Rajeshwari K, Sethi GR. Case report: isolated unilateral pulmonary vein atresia diagnosed on 128-slice multidetector CT. Indian J Radiol Imaging. 2011; 21:253–256.
Article23. Moore AD, Godwin JD, Dietrich PA, Verschakelen JA, Henderson WR Jr. Swyer-James syndrome: CT findings in eight patients. AJR Am J Roentgenol. 1992; 158:1211–1215.
Article24. Castañer E, Gallardo X, Ballesteros E, Andreu M, Pallardó Y, Mata JM, et al. CT diagnosis of chronic pulmonary thromboembolism. Radiographics. 2009; 29:31–50. ; discussion 50–53.
Article25. Moser KM, Olson LK, Schlusselberg M, Daily PO, Dembitsky WP. Chronic thromboembolic occlusion in the adult can mimic pulmonary artery agenesis. Chest. 1989; 95:503–508.
Article26. Castañer E, Alguersuari A, Gallardo X, Andreu M, Pallardó Y, Mata JM, et al. When to suspect pulmonary vasculitis: radiologic and clinical clues. Radiographics. 2010; 30:33–53.
Article27. Rossi SE, McAdams HP, Rosado-de-Christenson ML, Franks TJ, Galvin JR. Fibrosing mediastinitis. Radiographics. 2001; 21:737–757.
Article28. Friedman MJ, Gabor GE, Fishman MC, Griepp RB. Bilateral pulmonary artery stenosis associated with pericarditis. results of surgery and follow-up by magnetic resonance imaging. Chest. 1988; 93:883–885.29. Hwang YJ, Park CH, Jeon YB, Park KY. Severe pulmonary artery stenosis by a calcified pericardial ring. Eur J Cardiothorac Surg. 2006; 29:619–621.
Article30. Nguyen ET, Silva CI, Seely JM, Chong S, Lee KS, Müller NL. Pulmonary artery aneurysms and pseudoaneurysms in adults: findings at CT and radiography. AJR Am J Roentgenol. 2007; 188:W126–W134.
Article31. Simonneau G, Gatzoulis MA, Adatia I, Celermajer D, Denton C, Ghofrani A, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013; 62(25 Suppl):): D34-D41.
Article32. Grosse C, Grosse A. CT findings in diseases associated with pulmonary hypertension: a current review. Radiographics. 2010; 30:1753–1777.
Article33. Ng CS, Wells AU, Padley SP. A CT sign of chronic pulmonary arterial hypertension: the ratio of main pulmonary artery to aortic diameter. J Thorac Imaging. 1999; 14:270–278.
Article34. Lang IM, Madani M. Update on chronic thromboembolic pulmonary hypertension. Circulation. 2014; 130:508–518.
Article35. Saremi F, Gera A, Ho SY, Hijazi ZM, Sánchez-Quintana D. CT and MR imaging of the pulmonary valve. Radiographics. 2014; 34:51–71.
Article36. Ramachandran L, Dewan S, Kumar V, Wankhade B. Mucormycosis causing pulmonary artery aneurysm. Respir Med Case Rep. 2015; 16:71–73.
Article37. Ugolini P, Mousseaux E, Sadou Y, Sidi D, Mercier LA, Paquet E, et al. Idiopathic dilatation of the pulmonary artery: report of four cases. Magn Reson Imaging. 1999; 17:933–937.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Measurements of thoracic aorta and pulmonary artery diameter by computed tomography in normal Korean adults
- Three cases of right coronary anomaly confirmed by multi-detector computed tomography
- Overlooked or unrecognized pitfalls in noninvasive multi-detector computed tomography coronary angiography
- Multi-Detector CT Findings of Typical and Atypical Appendicitis: A Pictorial Essay
- MDCT Application in the Vascular System
