Analysis of Impingement between Patella Bone and Bearing Post in Cruciate-Substituting High-Flexion Total Knee Arthroplasty
- Affiliations
-
- 1Department of Orthopaedic Surgery, Sun Medical Center, Daejeon, Korea. bonjoolee@hanmail.net
- KMID: 2412340
- DOI: http://doi.org/10.4055/cios.2016.8.2.157
Abstract
- BACKGROUND
We investigated the causes of impingement between the patella bone and the bearing post during high flexion in cruciate-substituting total knee arthroplasty and proposed a treatment strategy.
METHODS
This prospective cohort study included 218 cases that had undergone cruciate-substituting total knee arthroplasty from February 2014 to January 2015; a single surgeon performed the operation using the same method without patellar resurfacing in all patients.
RESULTS
In these patients, the occurrence of impingement was determined by performing more than 120° high knee flexion after inserting a bearing perioperatively. The incidence of impingement was significantly associated with bearing design, femoral implant size, patella bone length, and patella inferior pole angle (p < 0.05). The impingement was resolved by resection of the lower articular side of the patella bone.
CONCLUSIONS
In the cruciate-substituting high-flexion total knee arthroplasty, impingement between the patella bone and bearing post was more common in patients with mobile bearing, small-size femoral component, and a long patella or a large inferior pole angle. In cases of intraoperative impingement between the patella bone and the bearing post, resection in the lower portion of the patella prevented impingement of the bearing with soft tissue or the patella by widening the space between the patella and the bearing post, which in turn prevented postoperative reduction in range of motion.
MeSH Terms
-
Aged
Aged, 80 and over
*Arthroplasty, Replacement, Knee/adverse effects/statistics & numerical data
Female
Humans
*Knee Prosthesis/adverse effects/statistics & numerical data
Male
Middle Aged
Patella/*physiopathology
*Postoperative Complications/epidemiology/physiopathology
Prospective Studies
Prosthesis Design
Range of Motion, Articular/physiology
Figure
-

Fig. 1 (A) The preoperative joint line was defined as a line through the midpoint of the lateral knee joint gap along the perpendicular line to the long axis of the fibula. (B) The postoperative joint line was defined as a line contacting the lowest point of the lateral femoral component along the perpendicular line to the long axis of the fibula. To find out the height of the joint line, we measured the distance from the top of the fibular head to the preoperative and postoperative joint line levels.
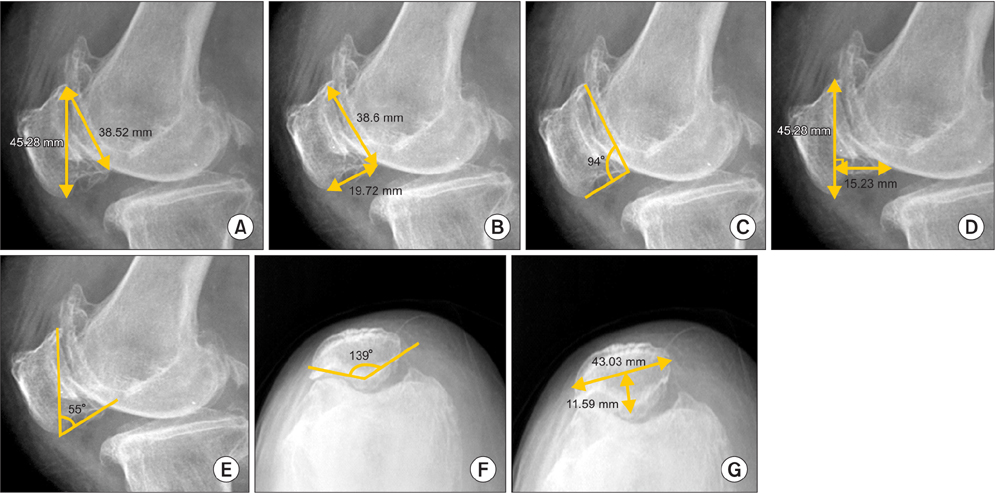
Fig. 2 (A) Patella length-articular ratio on the lateral view; we measured the ratio between patella long length from the superior pole to inferior pole and patella posterior articular length. (B) Patella nonarticular-articular ratio on the lateral view; we measured the ratio between posteroinferior nonarticular length and patella posterior articular length. (C) Patella articular-nonarticular angle on the lateral view; we measured the angle between posteroinferior nonarticular line and posterior articular line. (D) Patella long length and patella inner thickness ratio on the lateral view; we measured patella length as the distance from the superior pole to the inferior pole of the patella and the perpendicular distance from patella length to the posterior articular margin of the patella. (E) Patella inferior pole angle on the lateral view; we measured the angle between patella long length and posteroinferior nonarticular line. (F) Patella facet angle on the Merchant view; we measured the angle between medial and lateral articular margins of the patella. (G) Patella inner thickness ratio on the Merchant view; we measured the ratio between patella long length and perpendicular distance from patella length to the posterior articular margin of the patella.
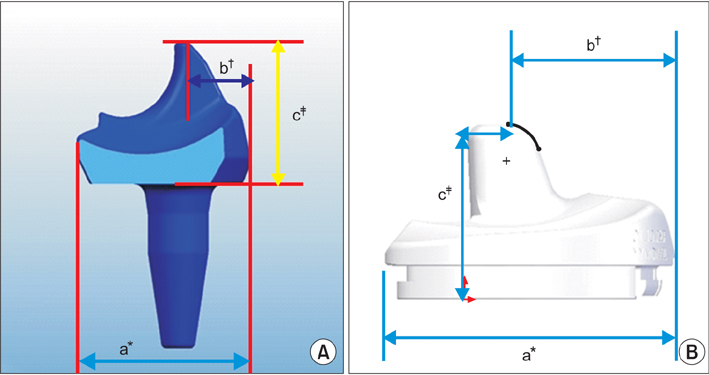
Fig. 3 The mobile bearing post was designed relatively anterior location and long length compared to the fixed bearing post. (A) Lateral aspect of the mobile type bearing. (B) Lateral aspect of the fixed type bearing. a*: anteroposterior distance of the bearing. b†: distance to the post position from the anterior margin of the bearing. c‡: height of the post.
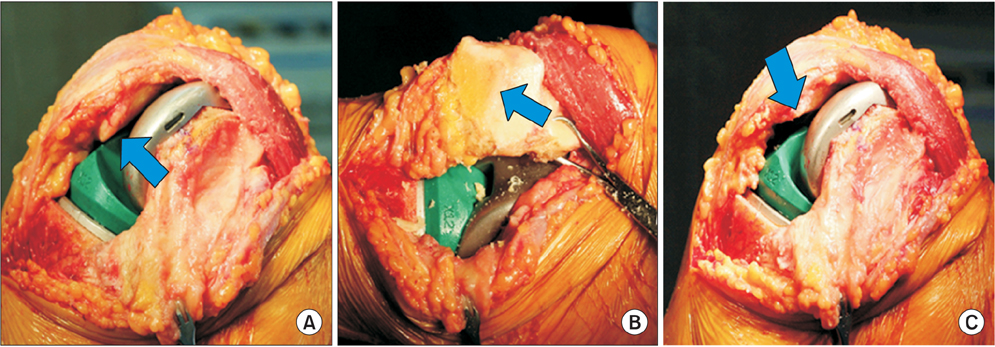
Fig. 4 (A) A 76-year-old female patient shows impingement (arrow) between patella bone and bearing post in cruciate-substituting high-flexion total knee arthroplasty. (B) We resected the lower patellar articular part (arrow) when impingement occurred. (C) Impingement disappeared (arrow) after lower patellar articular part resection.
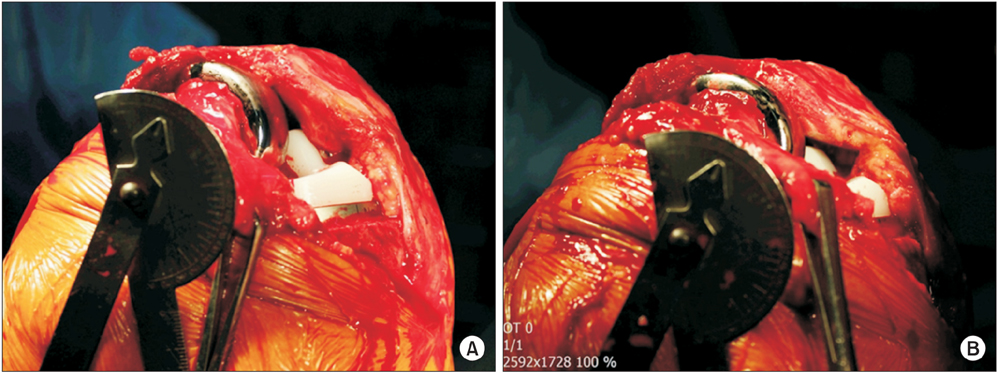
Fig. 5 The impingement between the patella bone and the bearing post causes forward displacement of the patella bone and forward displacement of the patella increases as knee flexion increases after impingement. (A) Forward displacement of the patella can lead to stretching of the patellofemoral ligament and retinaculum and reduction of the flexion gap. (B) Therefore, we treated cases with impingement by resection of the lower portion of the patella, and there was no occurrence of forward displacement of the patella.
Reference
-
1. Moynihan AL, Varadarajan KM, Hanson GR, et al. In vivo knee kinematics during high flexion after a posterior-substituting total knee arthroplasty. Int Orthop. 2010; 34(4):497–503.
Article2. Insall JN, Lachiewicz PF, Burstein AH. The posterior stabilized condylar prosthesis: a modification of the total condylar design. Two to four-year clinical experience. J Bone Joint Surg Am. 1982; 64(9):1317–1323.3. Kelly MA, Clarke HD. Long-term results of posterior cruciate-substituting total knee arthroplasty. Clin Orthop Relat Res. 2002; (404):51–57.
Article4. Li G, Most E, Otterberg E, et al. Biomechanics of posterior-substituting total knee arthroplasty: an in vitro study. Clin Orthop Relat Res. 2002; (404):214–225.
Article5. O'Rourke MR, Callaghan JJ, Goetz DD, Sullivan PM, Johnston RC. Osteolysis associated with a cemented modular posterior-cruciate-substituting total knee design: five to eight-year follow-up. J Bone Joint Surg Am. 2002; 84(8):1362–1371.6. Grigoris PH, Treacy RB, McMinn DJ. Patellotibial impingement in Kinemax stabilised total knee replacement. J Bone Joint Surg Br. 1992; 74(3):472–473.
Article7. Kramers-de Quervain IA, Engel-Bicik I, Miehlke W, Drobny T, Munzinger U. Fat-pad impingement after total knee arthroplasty with the LCS A/P-Glide system. Knee Surg Sports Traumatol Arthrosc. 2005; 13(3):174–178.
Article8. Macule F, Sastre S, Lasurt S, Sala P, Segur JM, Mallofre C. Hoffa's fat pad resection in total knee arthroplasty. Acta Orthop Belg. 2005; 71(6):714–717.9. Verborgt O, Victor J. Post impingement in posterior stabilised total knee arthroplasty. Acta Orthop Belg. 2004; 70(1):46–50.10. Patel DV, Aichroth PM, Wand JS. Posteriorly stabilised (Insall-Burstein) total condylar knee arthroplasty: a follow-up study of 157 knees. Int Orthop. 1991; 15(3):211–218.11. Selvarajah E, Hooper G. Restoration of the joint line in total knee arthroplasty. J Arthroplasty. 2009; 24(7):1099–1102.
Article12. Laskin RS. Management of the patella during revision total knee replacement arthroplasty. Orthop Clin North Am. 1998; 29(2):355–360.
Article13. Tang Q, Zhou Y, Yang D, Tang J, Shao H. The knee joint line position measured from the tibial side in Chinese people. J Arthroplasty. 2011; 26(7):989–993.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Joint Line Change in Posterior Cruciate Retained versus Cruciate Sacrificed Total Knee Aarthroplasty
- Results of Posterior Cruciate Retaining and Cruciate Substituting Total Knee Arthroplasty (3 to 8 years follow up)
- Influence of Patellar Tilt Angle in Merchant View on Postoperative Range of Motion in Posterior Cruciate Ligament-Substituting Fixed-Bearing Total Knee Arthroplasty
- Kinematics in Total Knee Arthroplasty
- Synovial Impingement after Total Knee Replacement Arthroplasty: A Case Report
