Yonsei Med J.
2018 Jun;59(4):501-510. 10.3349/ymj.2018.59.4.501.
Characteristics of Adrenal Incidentalomas in a Large, Prospective Computed Tomography-Based Multicenter Study: The COAR Study in Korea
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Inha University Hospital, Inha University School of Medicine, Incheon, Korea.
- 2Division of Endocrinology and Metabolism, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Division of Clinical Epidemiology and Biostatics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 4Division of Endocrinology and Metabolism, Gyeongsang National University Hospital, Gyeongsang National University School of Medicine, Jinju, Korea.
- 5Division of Endocrinology and Metabolism, Dong-A University Medical Center, Dong-A University College of Medicine, Busan, Korea.
- 6Division of Endocrinology and Metabolism, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. hun0108@amc.seoul.kr
- 7Division of Endocrinology and Metabolism, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea. skh2k@kuh.ac.kr
- KMID: 2410905
- DOI: http://doi.org/10.3349/ymj.2018.59.4.501
Abstract
- PURPOSE
Previous studies on adrenal incidentalomas (AIs) are limited by their retrospective design, small numbers of patients, Western populations, or use of an outdated imaging technique. We investigated the characteristics of AIs in Korean patients and compared them with those reported in the largest retrospective study in Italy to discover the effects of improved imaging techniques and ethnicity differences.
MATERIALS AND METHODS
This was a prospective, multicenter, cross-sectional observational study including 1005 Korean patients. Levels of plasma adrenocorticotrophic hormone, 24-h urinary free cortisol (UFC), serum cortisol after a 1 mg-dexamethasone suppression test, 24-h urinary fractionated metanephrine, and plasma aldosterone and plasma renin activity were measured. All AIs were characterized using computed tomography (CT).
RESULTS
Compared with the results of the Italian study, AIs in Korean patients were observed more frequently in men and predominantly on the left side. Korean patients with AIs were slightly younger, and fewer patients underwent surgery. Most AIs were nonfunctional in both studies, while fewer subclinical hypercortisolism and more primary aldosteronism (PA) cases were detected in Korean patients. In our study, high UFC levels showed very low sensitivity, compared to those in the Italian study. In pheochromocytoma or PA cases, there were no hormonal differences between the studies. AIs in Korean patients were smaller, such that a lower cutoff size for detecting adrenocortical carcinoma (ACC) could be warranted.
CONCLUSION
Recent advances in CT technology were leveraged to provide accurate characteristics of AIs and to detect smaller ACCs.
Keyword
MeSH Terms
Figure
-
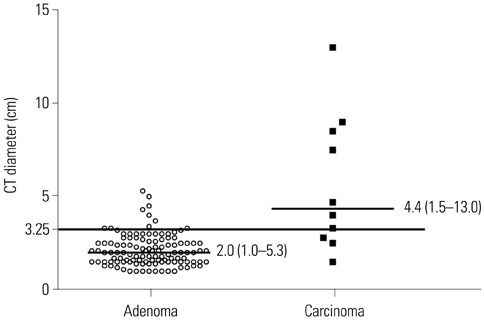
Fig. 1 Comparison of mass sizes of histologically proven adrenal cortical adenomas and carcinomas in the COAR cohort. Median values with ranges are shown. The cutoff value of 3.25 cm was determined according to the best cutoff values in receiver operating characteristics curves, corresponding to Youden's index.25 COAR, Co-work of Adrenal Research; CT, computed tomography.
Reference
-
1. Kloos RT, Gross MD, Francis IR, Korobkin M, Shapiro B. Incidentally discovered adrenal masses. Endocr Rev. 1995; 16:460–484.
Article2. Terzolo M, Stigliano A, Chiodini I, Loli P, Furlani L, Arnaldi G, et al. AME position statement on adrenal incidentaloma. Eur J Endocrinol. 2011; 164:851–870.
Article3. Arnaldi G, Boscaro M. Adrenal incidentaloma. Best Pract Res Clin Endocrinol Metab. 2012; 26:405–419.
Article4. Ambrosi B, Peverelli S, Passini E, Re T, Ferrario R, Colombo P, et al. Abnormalities of endocrine function in patients with clinically "silent" adrenal masses. Eur J Endocrinol. 1995; 132:422–428.
Article5. Androulakis II, Kaltsas G, Piaditis G, Grossman AB. The clinical significance of adrenal incidentalomas. Eur J Clin Invest. 2011; 41:552–560.
Article6. Nieman LK. Approach to the patient with an adrenal incidentaloma. J Clin Endocrinol Metab. 2010; 95:4106–4113.
Article7. Fassnacht M, Arlt W, Bancos I, Dralle H, Newell-Price J, Sahdev A, et al. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2016; 175:G1–G34.
Article8. Mantero F, Terzolo M, Arnaldi G, Osella G, Masini AM, Ali A, et al. A survey on adrenal incidentaloma in Italy. Study Group on Adrenal Tumors of the Italian Society of Endocrinology. J Clin Endocrinol Metab. 2000; 85:637–644.9. Kasperlik-Załuska AA, Otto M, Cichocki A, Rosłonowska E, Słowin´ska-Srzednicka J, Jeske W, et al. Incidentally discovered adrenal tumors: a lesson from observation of 1,444 patients. Horm Metab Res. 2008; 40:338–341.
Article10. Bhargav PR, Mishra A, Agarwal G, Agarwal A, Verma AK, Mishra SK. Adrenal incidentalomas: experience in a developing country. World J Surg. 2008; 32:1802–1808.
Article11. Bin X, Qing Y, Linhui W, Li G, Yinghao S. Adrenal incidentalomas: experience from a retrospective study in a Chinese population. Urol Oncol. 2011; 29:270–274.
Article12. Kim J, Bae KH, Choi YK, Jeong JY, Park KG, Kim JG, et al. Clinical characteristics for 348 patients with adrenal incidentaloma. Endocrinol Metab (Seoul). 2013; 28:20–25.
Article13. Comlekci A, Yener S, Ertilav S, Secil M, Akinci B, Demir T, et al. Adrenal incidentaloma, clinical, metabolic, follow-up aspects: single centre experience. Endocrine. 2010; 37:40–46.
Article14. Morelli V, Reimondo G, Giordano R, Della Casa S, Policola C, Palmieri S, et al. Long-term follow-up in adrenal incidentalomas: an Italian multicenter study. J Clin Endocrinol Metab. 2014; 99:827–834.
Article15. Yeomans H, Calissendorff J, Volpe C, Falhammar H, Mannheimer B. Limited value of long-term biochemical follow-up in patients with adrenal incidentalomas-a retrospective cohort study. BMC Endocr Disord. 2015; 15:6.
Article16. Cho YY, Suh S, Joung JY, Jeong H, Je D, Yoo H, et al. Clinical characteristics and follow-up of Korean patients with adrenal incidentalomas. Korean J Intern Med. 2013; 28:557–564.
Article17. Fu J, Festen EA, Wijmenga C. Multi-ethnic studies in complex traits. Hum Mol Genet. 2011; 20:R206–R213.
Article18. Morelli V, Donadio F, Eller-Vainicher C, Cirello V, Olgiati L, Savoca C, et al. Role of glucocorticoid receptor polymorphism in adrenal incidentalomas. Eur J Clin Invest. 2010; 40:803–811.
Article19. Siggelkow H, Etmanski M, Bozkurt S, Groβ P, Koepp R, Brockmoller J, et al. Genetic polymorphisms in 11β-hydroxysteroid dehydrogenase type 1 correlate with the postdexamethasone cortisol levels and bone mineral density in patients evaluated for osteoporosis. J Clin Endocrinol Metab. 2014; 99:E293–E302.
Article20. Suzuki Y, Sasagawa I, Suzuki H, Izumi T, Kaneko H, Nakada T. The role of ultrasonography in the detection of adrenal masses: comparison with computed tomography and magnetic resonance imaging. Int Urol Nephrol. 2001; 32:303–306.21. Tabarin A, Bardet S, Bertherat J, Dupas B, Chabre O, Hamoir E, et al. Exploration and management of adrenal incidentalomas. French Society of Endocrinology Consensus. Ann Endocrinol (Paris). 2008; 69:487–500.22. American Diabetes Association. Standards of medical care in diabetes--2013. Diabetes Care. 2013; 36:Suppl 1. S11–S66.23. WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004; 363:157–163.24. Kanis JA, Melton LJ 3rd, Christiansen C, Johnston CC, Khaltaev N. The diagnosis of osteoporosis. J Bone Miner Res. 1994; 9:1137–1141.
Article25. Youden WJ. Index for rating diagnostic tests. Cancer. 1950; 3:32–35.
Article26. Young WF Jr. Management approaches to adrenal incidentalomas. A view from Rochester, Minnesota. Endocrinol Metab Clin North Am. 2000; 29:159–185.27. Dunnick NR, Korobkin M. Imaging of adrenal incidentalomas: current status. AJR Am J Roentgenol. 2002; 179:559–568.
Article28. Song JH, Chaudhry FS, Mayo-Smith WW. The incidental adrenal mass on CT: prevalence of adrenal disease in 1,049 consecutive adrenal masses in patients with no known malignancy. AJR Am J Roentgenol. 2008; 190:1163–1168.
Article29. Blake MA, Kalra MK, Sweeney AT, Lucey BC, Maher MM, Sahani DV, et al. Distinguishing benign from malignant adrenal masses: multi-detector row CT protocol with 10-minute delay. Radiology. 2006; 238:578–585.
Article30. Foti G, Faccioli N, Mantovani W, Malleo G, Manfredi R, Mucelli RP. Incidental adrenal lesions: accuracy of quadriphasic contrast enhanced computed tomography in distinguishing adenomas from nonadenomas. Eur J Radiol. 2012; 81:1742–1750.
Article31. Kim HY, Kim SG, Lee KW, Seo JA, Kim NH, Choi KM, et al. Clinical study of adrenal incidentaloma in Korea. Korean J Intern Med. 2005; 20:303–309.
Article32. Tabuchi Y, Otsuki M, Kasayama S, Kosugi K, Hashimoto K, Yamamoto T, et al. Clinical and endocrinological characteristics of adrenal incidentaloma in Osaka region, Japan. Endocr J. 2016; 63:29–35.
Article33. Chiodini I. Clinical review: diagnosis and treatment of subclinical hypercortisolism. J Clin Endocrinol Metab. 2011; 96:1223–1236.34. Ito Y, Takeda R, Takeda Y. Subclinical primary aldosteronism. Best Pract Res Clin Endocrinol Metab. 2012; 26:485–495.
Article35. Barzon L, Sonino N, Fallo F, Palu G, Boscaro M. Prevalence and natural history of adrenal incidentalomas. Eur J Endocrinol. 2003; 149:273–285.
Article36. Stowasser M, Sharman J, Leano R, Gordon RD, Ward G, Cowley D, et al. Evidence for abnormal left ventricular structure and function in normotensive individuals with familial hyperaldosteronism type I. J Clin Endocrinol Metab. 2005; 90:5070–5076.
Article37. Funder JW, Carey RM, Fardella C, Gomez-Sanchez CE, Mantero F, Stowasser M, et al. Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2008; 93:3266–3281.
Article38. Nieman LK. Update on subclinical Cushing's syndrome. CurrOpin Endocrinol Diabetes Obes. 2015; 22:180–184.
Article39. Dackiw AP, Lee JE, Gagel RF, Evans DB. Adrenal cortical carcinoma. World J Surg. 2001; 25:914–926.
Article40. Hong AR, Kim JH, Park KS, Kim KY, Lee JH, Kong SH, et al. Optimal follow-up strategies for adrenal incidentalomas: reappraisal of the 2016 ESE-ENSAT guidelines in real clinical practice. Eur J Endocrino. 2017; 177:475–483.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Differential Diagnosis of Adrenal Mass Using Imaging Modality: Special Emphasis on F-18 Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography/Computed Tomography
- Utility of F-18 FDG-PET in Detecting Primary Aldosteronism in Patients with Bilateral Adrenal Incidentalomas
- Adrenal Incidentaloma: Imaging Approach and Differential Diagnosis
- Is Follow-up of Adrenal Incidentalomas Always Mandatory?
- Clinical Characteristics and Metabolic Features of Patients with Adrenal Incidentalomas with or without Subclinical Cushing's Syndrome
