Arthroscopy Techniques in Foot and Ankle Field: Arthroscopic Ankle and Subtalar Fusion
- Affiliations
-
- 1Department of Orthopedic Surgery, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea. ortho1@hanmail.net
- KMID: 2410058
- DOI: http://doi.org/10.4055/jkoa.2018.53.2.112
Abstract
- For the arthroscopic fusion procedure, the development of arthroscopic techniques of joint preparation for fusion have made arthroscopic ankle arthrodesis popular, and foot and ankle surgeons also have gained considerable experience in arthroscopic techniques. Arthroscopic techniques offer minimized soft tissue disruption, lower morbidity and mortality, faster recovery, and shorter hospital stay and time to fusion. In addition, they may reduce the risk of wound complications for patients with a poor soft tissue envelope or relevant co-morbidities.
Keyword
MeSH Terms
Figure
-

Figure 1 Before performing arthroscopic ankle arthrodesis, ankle anteroposterior (A), lateral (B), oblique view, routine foot series, lower extremity radiography and hindfoot alignment view (C) with weight bearing were taken to evaluate ankle joint, adjacent joint, status and degree of deformities.

Figure 2 Ankle distractor can be used to facilitate observation of ankle joint with arthroscope.
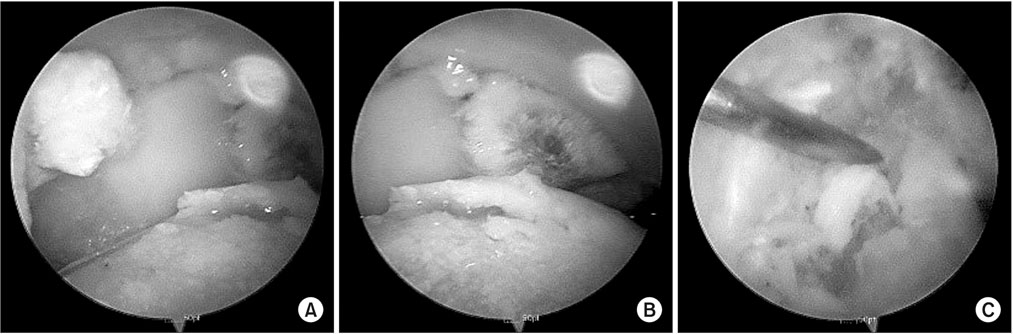
Figure 3 For successful fusion, bony spur and synovial membrane within operation field (A), fibrous tissue (B), and loose bodies (C) were removed to facilitate operative manipulation of arthroscope. Furthermore, subchondral bone and cartilage of talus and tibial plafond were removed to obtain enough contact surface between cancellous bones.

Figure 4 Because various screw fixation methods used in ankle fusion are for maximal compressive force, operators should select proper screw fixation method.

Figure 5 Because hindfoot joint pain may be somewhat ambigous and there are many structures that cause pain, targeted injection can be performed to access that cause of pain is subtalar joint or extraarticular structures of subtalar joint. It is important to confirm resolution of symptom after local targeted injection toward desired structures under fluoroscopy rather than blind technique.
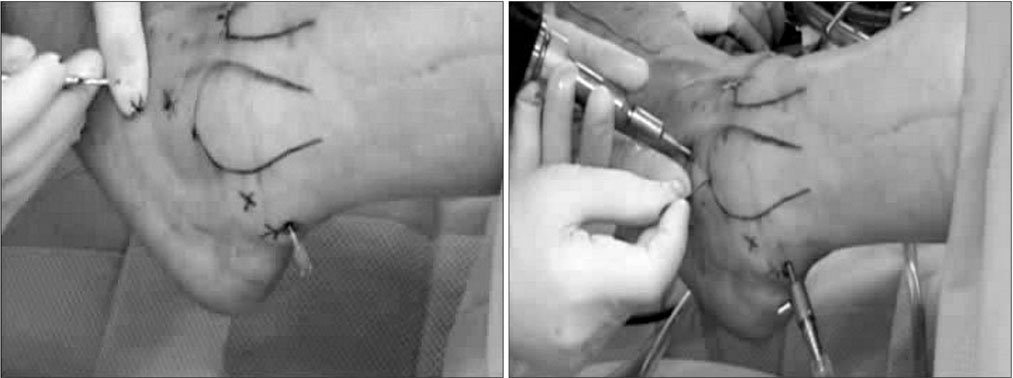
Figure 6 Anterolateral portal for arthroscopic subtalar fusion is 1.5 cm anterior to midline of fibula and 1 cm inferior to tip of lateral malleolus. Posterolateral portal is located at the level of distal end of fibula from lateral soft spot of Achilles tendon.

Figure 7 Unlike the ankle joint, Because subtalar joint is devided into posterior, middle, and anterior joint, operator should be well prepared for these articular surfaces when the subtalar joint is fused.

Figure 8 Usually, cannulated screws are inserted from posteroinferior aspect of calcaneus toward talar body. Until now, evidence for optimal location and number of screw to obtain good fusion rate is inadequate.

Figure 9 Fusion rate of arthroscopic subtalar fusion is reported to be excellent.
Reference
-
1. Grimes CA, Mungle CS, Zeng ZF, et al. Wireless magnetoelastic resonance sensors: a critical review. Sensors. 2002; 2:294–313.
Article2. O'Leary Z. The essential guide to doing research. . London: Sage;2004.3. Townshend D, Di Silvestro M, Krause F, et al. Arthroscopic versus open ankle arthrodesis: a multicenter comparative case series. J Bone Joint Surg Am. 2013; 95:98–102.
Article4. Myerson MS, Quill G. Ankle arthrodesis. A comparison of an arthroscopic and an open method of treatment. Clin Orthop Relat Res. 1991; 268:84–95.5. Michael JM, Golshani A, Gargac S, Goswami T. Biomechanics of the ankle joint and clinical outcomes of total ankle replacement. J Mech Behav Biomed Mater. 2008; 1:276–294.
Article6. Nielsen KK, Linde F, Jensen NC. The outcome of arthroscopic and open surgery ankle arthrodesis: a comparative retrospective study on 107 patients. Foot Ankle Surg. 2008; 14:153–157.7. Gougoulias NE, Agathgelidis FG, Parsons SW. Arthroscopic ankle arthrodesis. Foot Ankle Int. 2007; 28:695–706.
Article8. Dannawi Z, Nawabi DH, Patel A, Leong JJH, Moore DJ. Arthroscopic ankle arthrodesis: are results reproducible irrespective of pre-operative deformity? Foot Ankle Surg. 2011; 17:294–299.
Article9. Mazur JM, Schwartz E, Simon SR. Ankle arthrodesis: longterm follow-up with gait analysis. J Bone Joint Surg Am. 1979; 61:964–975.
Article10. Lynch AF, Bourne RB, Rorabeck CH. The long-term results of ankle arthrodesis. J Bone Joint Surg Br. 1988; 70:113–116.
Article11. Winson IG, Robinson DE, Allen PE. Arthroscopic ankle arthrodesis. J Bone Joint Surg Br. 2005; 87:343–347.
Article12. Schneider D. Arthroscopic ankle fusion. Arth Video J. 1983; 3.13. Peterson KS, Lee MS, Buddecke DE. Arthroscopic versus open ankle arthrodesis: a retrospective cost analysis. J Foot Ankle Surg. 2010; 49:242–247.
Article14. Chahal J, Stephen DJ, Bulmer B, Daniels T, Kreder HJ. Factors associated with outcome after subtalar arthrodesis. J Orthop Trauma. 2006; 20:555–561.
Article15. Easley ME, Trnka HJ, Schon LC, Myerson MS. Isolated subtalar arthrodesis. J Bone Joint Surg Am. 2000; 82:613–624.
Article16. Albert A, Deleu PA, Leemrijse T, Maldague P, Devos Bevernage B. Posterior arthroscopic subtalar arthrodesis: ten cases at one-year follow-up. Orthop Traumatol Surg Res. 2011; 97:401–405.
Article17. Amendola A, Lee KB, Saltzman CL, Suh JS. Technique and early experience with posterior arthroscopic subtalar arthrodesis. Foot Ankle Int. 2007; 28:298–302.
Article18. Chuckpaiwong B, Easley ME, Glisson RR. Screw placement in subtalar arthrodesis: a biomechanical study. Foot Ankle Int. 2009; 30:133–141.
Article19. Gosch C, Verrette R, Lindsey DP, Beaupré GS, Lehnert B. Comparison of initial compression force across the subtalar joint by two different screw fixation techniques. J Foot Ankle Surg. 2006; 45:168–173.
Article20. Hintermann B, Valderrabano V, Nigg B. Influence of screw type on obtained contact area and contact force in a cadaveric subtalar arthrodesis model. Foot Ankle Int. 2002; 23:986–991.
Article21. Walter R, Butler M, Parsons S. Arthroscopic subtalar arthrodesis through the two-portal sinus tarsi approach: a series of 77 cases. In : The BOFAS Annual Scientific Meeting; 2015 Nov 12; Guildford, England.22. Narita N, Takao M, Innami K, Kato H, Matsushita T. Minimally invasive subtalar arthrodesis with iliac crest autograft through posterior arthroscopic portals: a technical note. Foot Ankle Int. 2012; 33:803–805.
Article23. Lee KB, Park CH, Seon JK, Kim MS. Arthroscopic subtalar arthrodesis using a posterior 2-portal approach in the prone position. Arthroscopy. 2010; 26:230–238.
Article
