Role of common bile duct resection in T2 and T3 gallbladder cancer patients
- Affiliations
-
- 1Department of Surgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Surgery, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. kskim88@yuhs.ac
- 3Department of Surgery, Wonju Severance Christian Hospital, Yonsei University College of Medicine, Wonju, Korea.
- 4Department of Internal Medicine, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2409079
- DOI: http://doi.org/10.14701/ahbps.2018.22.1.42
Abstract
- BACKGROUNDS/AIMS
Routine bile duct resection as part of the typical oncological resection for patients with advanced gallbladder cancer remains controversial with regard to, ultimately, curative value. The aim of this study was to compare oncological outcomes for patients undergoing surgery for gallbladder cancer with or without bile duct resection.
METHODS
We recruited, for the purpose of this study, all patients who underwent surgical resection for T2 and T3 gallbladder cancer at Severance hospital, Seoul, Korea, during the period January 2000 and December of 2011. The patient data was reviewed retrospectively.
RESULTS
The patients (n=149) recruited to participate in the study were divided into two groups according to their bile duct resection status: The bile duct resection group (BDR group, n=54); and, the bile duct non-resection group (BDNR group, n=95). Significant difference was found in lymph node retrieval between BDR and BDNR groups (15 vs. 5, respectively with p < 0.001). There was no significant difference between the two groups with regard to the five year survival rate (43% in BDR group vs. 57% in BDNR group, p=0.339). Following multivariate analysis, lymph node metastasis, advanced T-stage, and total retrieved lymph nodes <6 were independent prognostic factors for poor survival in patients with T2 and T3 gallbladder cancer.
CONCLUSIONS
The findings revealed by the current study suggest that the role of bile duct resection might be limited to improved staging, and offers no advantage in long-term survival. However, in view of the foregoing and given the minimal increase in morbidity associated with BDR, it should be actively considered as a treatment option for patients who present with findings suspicious for invasion around hepatoduodenal ligament.
MeSH Terms
Figure
-
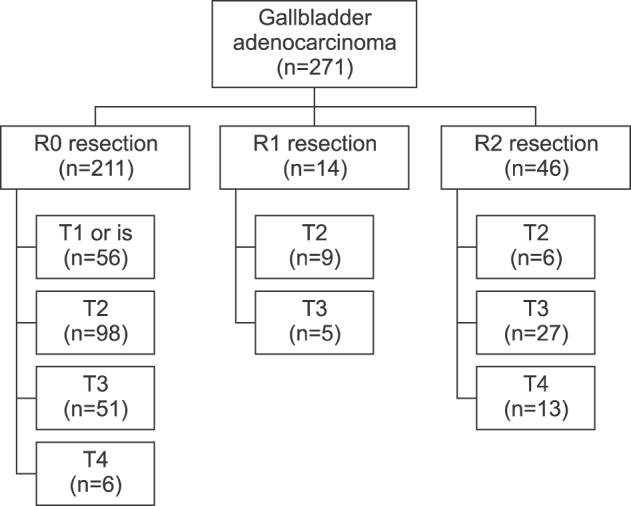
Fig. 1 Distribution of T-stage according to residual tumor.
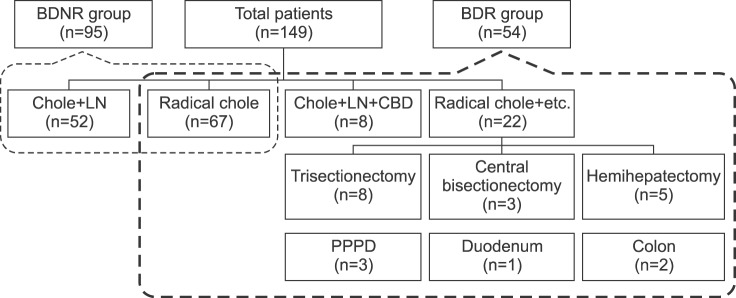
Fig. 2 Type of operative procedures. BDNR group, bile duct non-resection group; BDR group, bile duct resection group; Chole, cholecystectomy; LN, lymph node dissection; CBD, common bile duct resection; Radical chole+etc., Radical cholecystectomy and combined resection; PPPD, Pylorus-preserving pancreaticoduodenectomy.
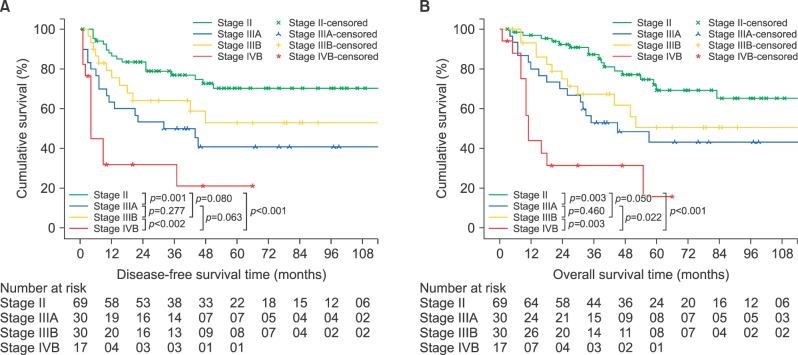
Fig. 3 Survival curves according to American Joint Committee on Cancer Staging Manuam 7th edition TNM stage. (A) Disease-free survival. (B) Overall survival.
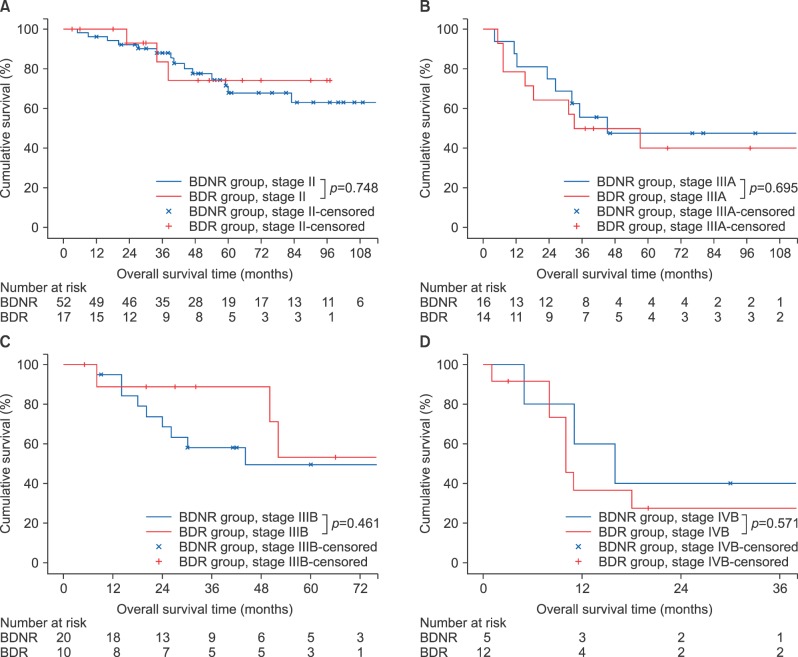
Fig. 4 Survival curves comparing the BDR and BDNR groups. (A) Overall survival for Stage II. (B) Overall survival for Stage IIIA. (C) Overall survival for Stage IIIB. (D) Overall survival for Stage IVB. BDNR group, Bile duct non-resection group; BDR group, Bile duct resection group.
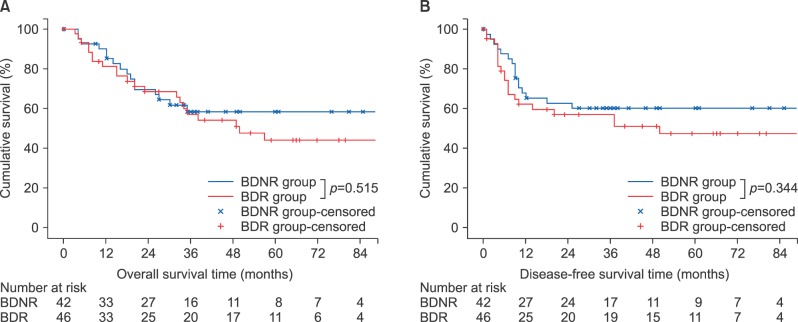
Fig. 5 Survival curves comparing the BDR and BDNR groups for liver resection patients. (A) Overall survival. (B) Disease-free survival. BDNR group, Bile duct non-resection group; BDR group, Bile duct resection group.
Reference
-
1. Lazcano-Ponce EC, Miquel JF, Muñoz N, Herrero R, Ferrecio C, Wistuba II, et al. Epidemiology and molecular pathology of gallbladder cancer. CA Cancer J Clin. 2001; 51:349–364. PMID: 11760569.
Article2. Hueman MT, Vollmer CM Jr, Pawlik TM. Evolving treatment strategies for gallbladder cancer. Ann Surg Oncol. 2009; 16:2101–2115. PMID: 19495882.
Article3. Ito H, Ito K, D'Angelica M, Gonen M, Klimstra D, Allen P, et al. Accurate staging for gallbladder cancer: implications for surgical therapy and pathological assessment. Ann Surg. 2011; 254:320–325. PMID: 21617582.4. Higuchi R, Ota T, Araida T, Kajiyama H, Yazawa T, Furukawa T, et al. Surgical approaches to advanced gallbladder cancer: a 40-year single-institution study of prognostic factors and resectability. Ann Surg Oncol. 2014; 21:4308–4316. PMID: 25023547.5. Benson AB 3rd, Abrams TA, Ben-Josef E, Bloomston PM, Botha JF, Clary BM, et al. NCCN clinical practice guidelines in oncology: hepatobiliary cancers. J Natl Compr Canc Netw. 2009; 7:350–391. PMID: 19406039.6. Araida T, Higuchi R, Hamano M, Kodera Y, Takeshita N, Ota T, et al. Should the extrahepatic bile duct be resected or preserved in R0 radical surgery for advanced gallbladder carcinoma? Results of a Japanese Society of Biliary Surgery Survey: a multicenter study. Surg Today. 2009; 39:770–779. PMID: 19779773.
Article7. Kokudo N, Makuuchi M, Natori T, Sakamoto Y, Yamamoto J, Seki M, et al. Strategies for surgical treatment of gallbladder carcinoma based on information available before resection. Arch Surg. 2003; 138:741–750. discussion 750. PMID: 12860755.
Article8. Sakamoto Y, Kosuge T, Shimada K, Sano T, Hibi T, Yamamoto J, et al. Clinical significance of extrahepatic bile duct resection for advanced gallbladder cancer. J Surg Oncol. 2006; 94:298–306. PMID: 16917876.
Article9. Choi SB, Han HJ, Kim WB, Song TJ, Suh SO, Choi SY. Surgical strategy for T2 and T3 gallbladder cancer: is extrahepatic bile duct resection always necessary? Langenbecks Arch Surg. 2013; 398:1137–1144. PMID: 24057276.
Article10. Lim H, Seo DW, Park DH, Lee SS, Lee SK, Kim MH, et al. Prognostic factors in patients with gallbladder cancer after surgical resection: analysis of 279 operated patients. J Clin Gastroenterol. 2013; 47:443–448. PMID: 23188077.11. Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009; 250:187–196. PMID: 19638912.12. Yoshikawa T, Sasako M, Sano T, Nashimoto A, Kurita A, Tsujinaka T, et al. Stage migration caused by D2 dissection with para-aortic lymphadenectomy for gastric cancer from the results of a prospective randomized controlled trial. Br J Surg. 2006; 93:1526–1529. PMID: 17051601.13. Pawlik TM, Gleisner AL, Cameron JL, Winter JM, Assumpcao L, Lillemoe KD, et al. Prognostic relevance of lymph node ratio following pancreaticoduodenectomy for pancreatic cancer. Surgery. 2007; 141:610–618. PMID: 17462460.
Article14. Kim YW, Kim NK, Min BS, Lee KY, Sohn SK, Cho CH, et al. The prognostic impact of the number of lymph nodes retrieved after neoadjuvant chemoradiotherapy with mesorectal excision for rectal cancer. J Surg Oncol. 2009; 100:1–7. PMID: 19418495.
Article15. Ito M, Mishima Y, Sato T. An anatomical study of the lymphatic drainage of the gallbladder. Surg Radiol Anat. 1991; 13:89–104. PMID: 1925922.
Article16. Kijima H, Wu Y, Yosizawa T, Suzuki T, Tsugeno Y, Haga T, et al. Pathological characteristics of early to advanced gallbladder carcinoma and extrahepatic cholangiocarcinoma. J Hepatobiliary Pancreat Sci. 2014; 21:453–458. PMID: 24591403.
Article17. Shimizu Y, Ohtsuka M, Ito H, Kimura F, Shimizu H, Togawa A, et al. Should the extrahepatic bile duct be resected for locally advanced gallbladder cancer. Surgery. 2004; 136:1012–1017. discussion 1018. PMID: 15523394.
Article18. Ogura Y, Tabata M, Kawarada Y, Mizumoto R. Effect of hepatic invasion on the choice of hepatic resection for advanced carcinoma of the gallbladder: histologic analysis of 32 surgical cases. World J Surg. 1998; 22:262–266. discussion 266-267. PMID: 9494418.
Article19. Jung SJ, Woo SM, Park HK, Lee WJ, Han MA, Han SS, et al. Patterns of initial disease recurrence after resection of biliary tract cancer. Oncology. 2012; 83:83–90. PMID: 22777276.
Article20. Jarnagin WR, Ruo L, Little SA, Klimstra D, D'Angelica M, DeMatteo RP, et al. Patterns of initial disease recurrence after resection of gallbladder carcinoma and hilar cholangiocarcinoma: implications for adjuvant therapeutic strategies. Cancer. 2003; 98:1689–1700. PMID: 14534886.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Should the Extrahepatic Bile Duct be Resected for T2 Gallbladder Cancer?
- Laparoscopic cholecystectomy and common bile duct exploration for gallstone and common bile duct stone in a patient with a left-sided gallbladder: a case report
- Clinical Review of Carcinomas of the Extrahepatic Bile Ducts and Gallbladders
- Introduction of 7th AJCC Cancer Staging: Gallbladder, Perihilar Bile Duct and Distal Common Bile Duct
- Laparoscopic radical cholecystectomy with common bile duct resection for T2 gallbladder cancer
