Prognostic Utility of Histological Growth Patterns of Colorectal Lung Oligometastasis
- Affiliations
-
- 1Department of Pathology, Dong-A University College of Medicine, Busan, Korea. msroh@dau.ac.kr
- 2Department of Pathology, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea.
- 3Department of Pathology, Gachon University of Medicine and Science, Incheon, Korea.
- KMID: 2408510
- DOI: http://doi.org/10.4132/jptm.2017.12.27
Abstract
- BACKGROUND
Patients with resectable colorectal lung oligometastasis (CLOM) demonstrate a heterogeneous oncological outcome. However, the parameters for predicting tumor aggressiveness have not yet been fully investigated in CLOM. This study was performed to determine the prognostic value of histological growth patterns in patients who underwent surgery for CLOM.
METHODS
The study included 92 patients who were diagnosed with CLOM among the first resection cases. CLOMs grow according to three histological patterns: aerogenous, pushing, and desmoplastic patterns. The growth patterns were evaluated on archival hematoxylin and eosin-stained tissue sections.
RESULTS
The aerogenous pattern was found in 29.4% (n=27) of patients, the pushing pattern in 34.7% (n=32), the desmoplastic pattern in 6.5% (n=6), and a mix of two growth patterns in 29.4% (n=27). The size of the aerogenous pattern was significantly smaller than that of metastases with other patterns (p=.033). Kaplan-Meier analysis demonstrated that patients showing an aerogenous pattern appeared to have a poorer prognosis, which was calculated from the time of diagnosis of the CLOM (p=.044). The 5-year survival rate from the diagnosis of colorectal cancer tended to be lower in patients with an aerogenous pattern than in those who had a non-aerogenous pattern; however, the difference was marginally significant (p=.051). In the multivariate Cox analysis, the aerogenous pattern appeared as an independent predictor of poor overall survival (hazard ratio, 3.122; 95% confidence interval, 1.196 to 8.145; p=.020).
CONCLUSIONS
These results suggest that the growth patterns may play a part as a histology-based prognostic parameter for patients with CLOM.
Keyword
MeSH Terms
Figure
-

Fig. 1. Representative histologic features of the three different growth patterns of lung oligometastasis from colorectal adenocarcinoma. (A, B) In the aerogenous pattern, tumor clusters, nests, or single tumor cells spread into the air spaces of the lung parenchyma surrounding the edge of the tumor without destruction of the lung architecture, desmoplastic stroma, or inflammatory infiltrate. (C, D) In the pushing pattern, the metastasis grows by compression of the lung parenchyma, running parallel to the tumor-lung interface without desmoplastic stroma, and with only a mild inflammatory infiltrate. (E, F) In the desmoplastic pattern, the metastatic tumor is separated from the lung parenchyma by a desmoplastic rim infiltrated with lymphocytes. There is no direct contact between the tumor cells and lung parenchyma.
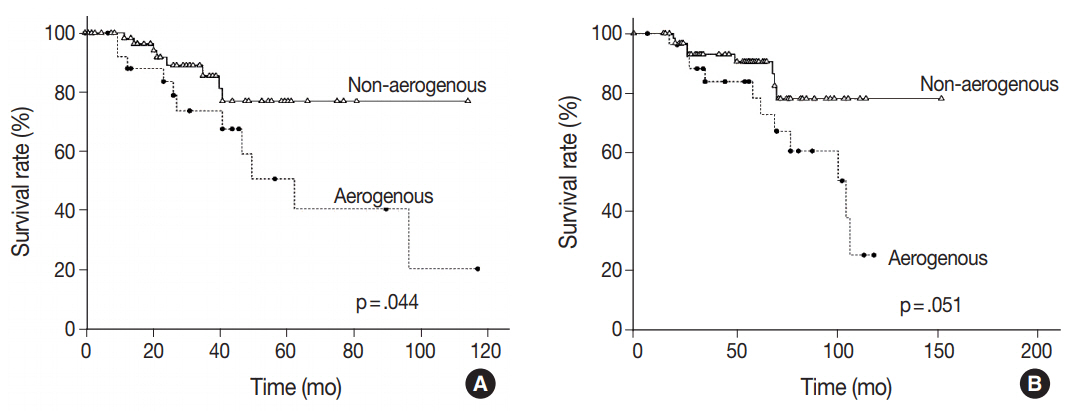
Fig. 2. Kaplan-Meier curves illustrating the overall survival of patients with colorectal lung oligometastasis (CLOM) in relation to growth patterns. (A) The overall survival rate calculated from the diagnosis of CLOM shows a shorter survival time in patients with CLOM having an aerogenous pattern than in those with CLOM having a non-aerogenous pattern (p=.044). (B) Although the difference was marginally significant (p=.051), the overall survival rate calculated from the time of diagnosis of colorectal cancer tends to show a shorter survival length in patients with CLOM having an aerogenous pattern than in those with CLOM with a non-aerogenous pattern.
Reference
-
1. Weichselbaum RR, Hellman S. Oligometastases revisited. Nat Rev Clin Oncol. 2011; 8:378–82.
Article2. Corbin KS, Hellman S, Weichselbaum RR. Extracranial oligometastases: a subset of metastases curable with stereotactic radiotherapy. J Clin Oncol. 2013; 31:1384–90.
Article3. Comito T, Cozzi L, Clerici E, et al. Stereotactic ablative radiotherapy (SABR) in inoperable oligometastatic disease from colorectal cancer: a safe and effective approach. BMC Cancer. 2014; 14:619.
Article4. Inoue M, Ohta M, Iuchi K, et al. Benefits of surgery for patients with pulmonary metastases from colorectal carcinoma. Ann Thorac Surg. 2004; 78:238–44.
Article5. Rama N, Monteiro A, Bernardo JE, Eugénio L, Antunes MJ. Lung metastases from colorectal cancer: surgical resection and prognostic factors. Eur J Cardiothorac Surg. 2009; 35:444–9.
Article6. Pfannschmidt J, Dienemann H, Hoffmann H. Surgical resection of pulmonary metastases from colorectal cancer; a systemic review of published series. Ann Thorac Surg. 2007; 84:324–38.7. Mitry E, Guiu B, Cosconea S, Jooste V, Faivre J, Bouvier AM. Epidemiology, management and prognosis of colorectal cancer with lung metastases: a 30-year population-based study. Gut. 2010; 59:1383–8.
Article8. Lee KS, Nam SK, Koh J, et al. Stromal expression of microRNA-21 in advanced colorectal cancer patients with distant metastases. J Pathol Transl Med. 2016; 50:270–7.
Article9. Iizasa T, Suzuki M, Yoshida S, et al. Prediction of prognosis and surgical indications for pulmonary metastasectomy from colorectal cancer. Ann Thorac Surg. 2006; 82:254–60.
Article10. Shiono S, Ishii G, Nagai K, et al. Histopathologic prognostic factors in resected colorectal lung metastases. Ann Thorac Surg. 2005; 79:278–82.
Article11. Vermeulen PB, Colpaert C, Salgado R, et al. Liver metastases from colorectal adenocarcinomas grow in three patterns with different angiogenesis and desmoplasia. J Pathol. 2001; 195:336–42.
Article12. Van den Eynden GG, Bird NC, Majeed AW, Van Laere S, Dirix LY, Vermeulen PB. The histological growth pattern of colorectal cancer liver metastases has prognostic value. Clin Exp Metastasis. 2012; 29:541–9.
Article13. Nielsen K, Rolff HC, Eefsen RL, Vainer B. The morphological growth patterns of colorectal liver metastases are prognostic for overall survival. Mod Pathol. 2014; 27:1641–8.
Article14. Nagashima I, Oka T, Hamada C, Naruse K, Osada T, Muto T. Histopathological prognostic factors influencing long-term prognosis after surgical resection for hepatic metastases from colorectal cancer. Am J Gastroenterol. 1999; 94:739–43.
Article15. Lunevicius R, Nakanishi H, Ito S, et al. Clinicopathological significance of fibrotic capsule formation around liver metastasis from colorectal cancer. J Cancer Res Clin Oncol. 2001; 127:193–9.
Article16. Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG. WHO classification of tumours of the lung, pleura, thymus and heart. 4th ed. Lyon: IARC Press;2015.17. Dai C, Xie H, Su H, et al. Tumor spread through air spaces affects the recurrence and overall survival in patients with lung adenocarcinoma > 2 to 3 cm. J Thorac Oncol. 2017; 12:1052–60.18. Paku S. Current concepts of tumor-induced angiogenesis. Pathol Oncol Res. 1998; 4:62–75.
Article19. Ueno H, Konishi T, Ishikawa Y, et al. Histological categorization of fibrotic cancer stroma in the primary tumor is an independent prognostic index in resectable colorectal liver metastasis. Am J Surg Pathol. 2014; 38:1380–6.20. Eefsen RL, Van den Eynden GG, Høyer-Hansen G, et al. Histopathological growth pattern, proteolysis and angiogenesis in chemonaive patients resected for multiple colorectal liver metastases. J Oncol. 2012; 2012:907971.
Article21. Terayama N, Terada T, Nakanuma Y. Histologic growth patterns of metastatic carcinomas of the liver. Jpn J Clin Oncol. 1996; 26:24–9.
Article22. Warth A. Spread through air spaces (STAS): a comprehensive update. Transl Lung Cancer Res. 2017; 6:501–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Complete response to local therapy for advanced hepatocellular carcinoma with lung metastasis: a case report
- Lung Metastasis of Colorectal Cancer
- Local ablative radiotherapy for oligometastatic non-small cell lung cancer
- Comparative Analysis of Clinicopathologic Features and Tumor Suppressor Genes Expression According to Growth Patterns in Colorectal Carcinomas
- Correlation between Expression of c-erbB-2 Oncogene and Various Prognostic Factors in the Colorectal Carcinoma
