Leukocytoclastic Vasculitis of the Breast: A Case Report
- Affiliations
-
- 1Department of Radiology, Ajou University School of Medicine, Suwon, Korea. h219435@gmail.com
- 2Department of Pathology, Ajou University School of Medicine, Suwon, Korea.
- KMID: 2407933
- DOI: http://doi.org/10.3348/jksr.2018.78.4.279
Abstract
- Leukocytoclastic vasculitis is a rare disease characterized by neutrophil and immune-complex deposition in the small vessel walls. We report a 47-year-old female patient with leukocytoclastic vasculitis of the breast, presenting as breast edema on mammography, irregular hypoechoic lesion with central necrosis on ultrasonography and regionally distributed heterogeneous non-mass enhancement on magnetic resonance imaging.
MeSH Terms
Figure
-
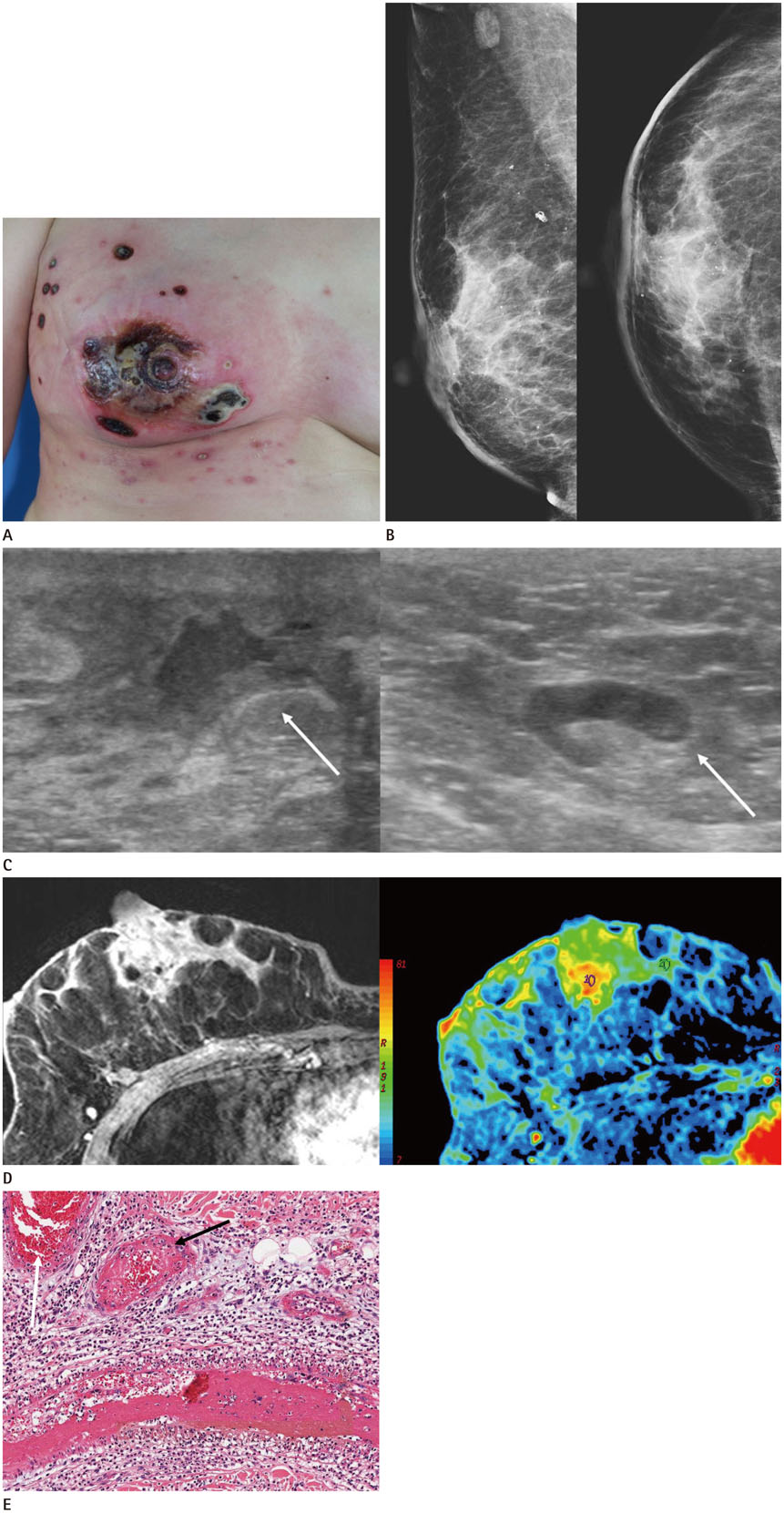
Fig. 1 A 47-year-old woman with leukocytoclastic vasculitis of right breast. A. Patient showing erythematous skin changes, ulceration and necrosis of right breast. B. Mammographic images show focal asymmetry in the subareolar area with diffuse skin thickening and trabecular thickening of right breast. C. Ultrasound shows the presence of an irregular hypoechoic lesion with central necrosis (an arrow in the left image) in the right subareolar area. Reactive lymph node hyperplasia (an arrow in the right image) is noted in right axilla. D. The contrast-enhanced fat-suppressed T1-weighted image reveals regionally distributed heterogeneous non-mass enhancement in the right central breast with involvement of the right nipple and periareolar area (left). Color map image obtained with computer-aided diagnosis (right), shows the lesion containing a central red portion suggesting initial rapid and delayed washout pattern of kinetic analysis. E. Histological examination (hematoxylin and eosin stain, × 100) reveals several infiltrating neutrophils in the small vessel wall causing vessel wall damage (black arrow). Massive intravascular fibrin thrombi are also noted in the superficial vessels (white arrow).
Reference
-
1. Fiorentino DF. Cutaneous vasculitis. J Am Acad Dermatol. 2003; 48:311–340.
Article2. Dubost JJ, Souteyrand P, Sauvezie B. Drug-induced vasculitides. Baillieres Clin Rheumatol. 1991; 5:119–138.
Article3. Hernández-Rodríguez J, Hoffman GS. Updating single-organ vasculitis. Curr Opin Rheumatol. 2012; 24:38–45.
Article4. Kadotani Y, Enoki Y, Itoi N, Kojima F, Kato G, Lee CJ. Giant cell arteritis of the breast: a case report with a review of literatures. Breast Cancer. 2010; 17:225–232.
Article5. Khalil HH, Marsden J, Akbar N, Gordon P, Roberts J, Schulte KM. Polyarteritis nodosa of the breast: presentation and management. Int J Surg. 2009; 7:446–450.
Article6. Szabo-Moskal J. Wegener's granulomatosis of the breast: a case report. Pol J Radiol. 2014; 79:117–119.
Article7. Lee JY, Joo M. Isolated breast vasculitis manifested as breast edema with suggestive sonographic findings: a case report with imaging findings. J Med Ultrason. 2017; 44:191–195.
Article8. Ozturk M, Mavili E, Kahriman G, Akcan AC, Ozturk F. Granulomatous mastitis: radiological findings. Acta Radiol. 2007; 48:150–155.
Article9. Chu AN, Seiler SJ, Hayes JC, Wooldridge R, Porembka JH. Magnetic resonance imaging characteristics of granulomatous mastitis. Clin Imaging. 2017; 43:199–201.
Article10. Sunderkötter C, Bonsmann G, Sindrilaru A, Luger T. Management of leukocytoclastic vasculitis. J Dermatolog Treat. 2005; 16:193–206.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Leukocytoclastic Vasculitis Following COVID-19 Vaccination
- Warfarin-induced Leukocytoclastic Vasculitis
- Sibutramine (Reductil(R))-Induced Cutaneous Leukocytoclastic Vasculitis: A Case Report
- A Case of Annular Leukocytoclastic Vasculitis
- A Case of Leukocytoclastic Vasculitis Associated with Pulmonary Tuberculosis
