Low-Dose Unenhanced Computed Tomography with Iterative Reconstruction for Diagnosis of Ureter Stones
- Affiliations
-
- 1Department of Urology, College of Medicine, Chung-Ang University, Seoul, Korea.
- 2Department of Emergency Medicine, College of Medicine, Chung-Ang University, Seoul, Korea. emdhlee@cau.ac.kr
- 3Department of Radiology, College of Medicine, Chung-Ang University, Seoul, Korea.
- 4Chung-Ang University School of Medicine, Seoul, Korea.
- KMID: 2407862
- DOI: http://doi.org/10.3349/ymj.2018.59.3.389
Abstract
- PURPOSE
To study the clinical application of low-dose unenhanced computed tomography with iterative reconstruction technique (LDCT-IR) on renal colic in the emergency department.
MATERIALS AND METHODS
We conducted a prospective, single-blinded, randomized, and non-inferiority study. From March 2014 to August 2015, 112 patients with renal colic were included, and were randomized to either LDCT-IR (n=46) or standard-dose unenhanced CT (SDCT) (n=66) groups. The accuracy of urolithiasis diagnosis was the primary endpoint of this study. Radiation dose, size and location of the stone, hydronephrosis, other diseases except urolithiasis, and results of treatment were analyzed between the two groups.
RESULTS
The average effective dose radiation of SDCT was approximately four times higher than that of LDCT-IR (6.52 mSv vs. 1.63 mSv, p < 0.001). There was no significant difference in the accuracy of ureteral stone diagnosis between the two groups (LDCT-IR group: 96.97% vs. SDCT group: 98.96%, p=0.392). No significant difference was observed regarding the size and location of a stone, hydronephrosis, and diagnosis of other diseases, except urolithiasis. False negative results were found in two LDCT-IR patients and in one SDCT patient. In these patients, stones were misread as vascular calcification, and were difficult to diagnose because evidence of hydronephrosis and ureteral dilatation was not found.
CONCLUSION
LDCT-IR, as a first-line imaging test, was non-inferior to SDCT with respect to diagnosis of ureter stones, and was clinically available for the evaluation of renal colic.
Keyword
MeSH Terms
Figure
-
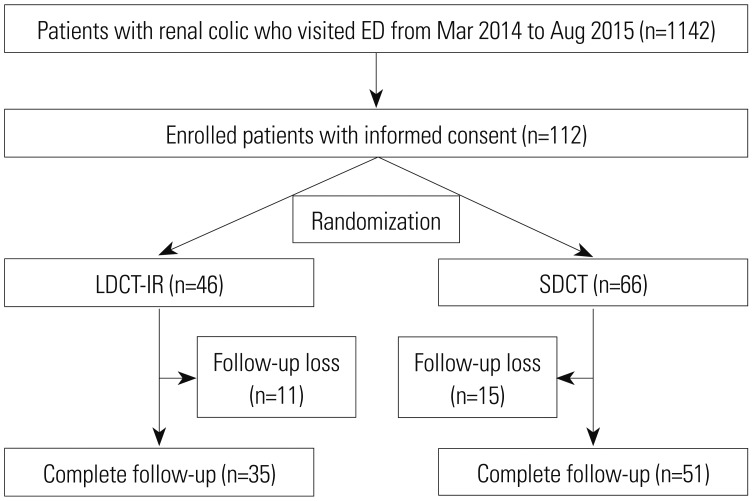
Fig. 1 Flow chart of the patient inclusion and review protocol. ED, emergency department; LDCT-IR, low-dose unenhanced computed tomography with iterative reconstruction technique; SDCT, standard-dose unenhanced computed tomography.
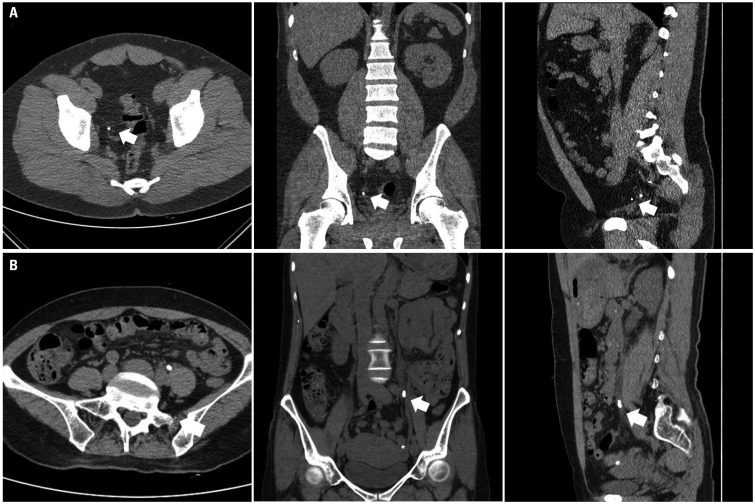
Fig. 2 A comparison between LDCT-IR and SDCT for a ureter stone. (A) LDCT-IR sets (axial, coronal, and sagittal images) of a 35-year-old man with a right lower ureteral stone (white arrows). The body mass index of the patient was 34.3 kg/m2, and the effective radiation dose was 3.384 mSv. (B) SDCT sets (axial, coronal, and sagittal images) of a 50-year-old woman with a left upper ureteral stone (white arrows). The body mase index of the patient was 20.8 kg/m2, and the effective radiation dose was 4.416 mSv. LDCT-IR, low-dose computed tomography with iterative reconstruction technique; SDCT, standard-dose unenhanced computed tomography.
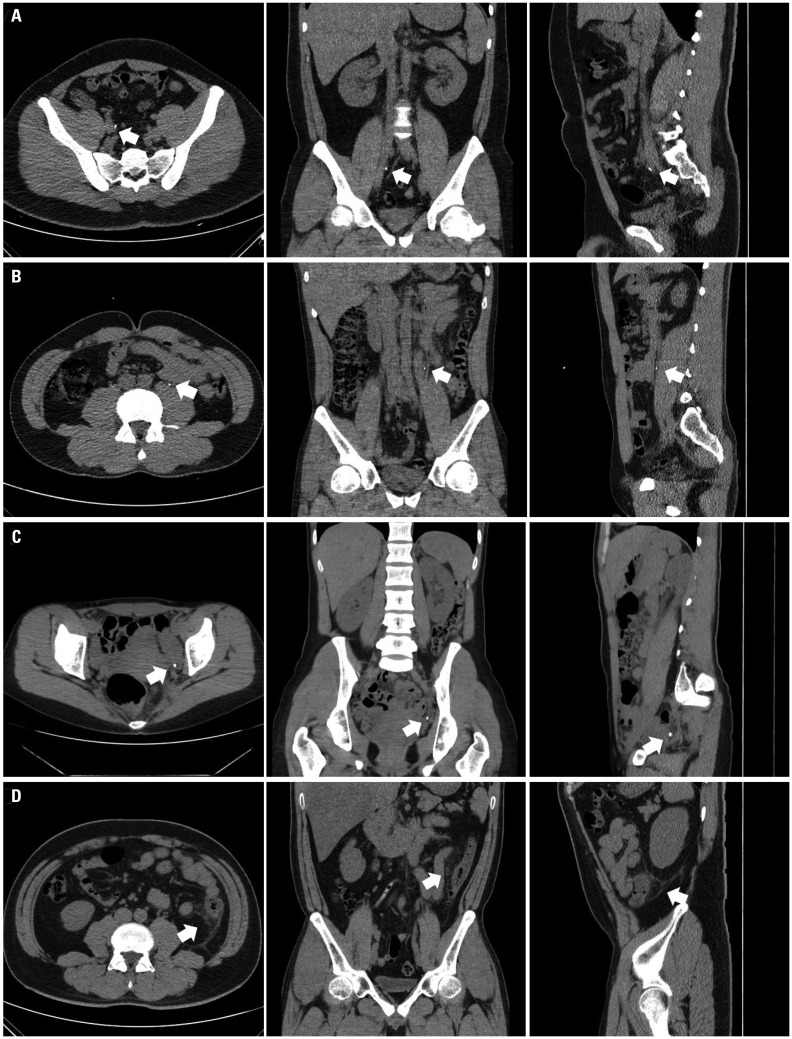
Fig. 3 LDCT-IR and SDCT for false negative findings for ureter stone and causes other than ureter stone. (A) LDCT-IR sets (axial, coronal, and sagittal images) of a 21-year-old man with a right mid ureteral stone (white arrows). The radiologist did not discriminate between a ureter stone and vascular calcification. (B) LDCT-IR sets (axial, coronal, and sagittal images) of a 40-year-old man with a left mid ureteral stone (white arrows). The radiologist discriminated it as a vascular calcification rather than as a ureter stone. (C) SDCT sets (axial, coronal, and sagittal images) of a 33-year-old woman with a left lower ureteral stone (white arrows). The radiologist discriminated the calcification because there was no ureteral dilatation and no ureteral course tracking. (D) SDCT sets (axial, coronal, and sagittal images) of a 40-year-old man who complained of left flank pain. The radiologist discriminated the several diverticula in D-colon with pericolic infiltration (white arrows) and no urinary stone. The final diagnosis of left flank pain was acute diverticulitis. LDCT-IR, low-dose computed tomography with iterative reconstruction technique; SDCT, standard-dose unenhanced computed tomography.
Reference
-
1. Chi BH, Chang IH, Choi SY, Suh DC, Chang CW, Choi YJ, et al. Daily mean temperature and urolithiasis presentation in six cities in Korea: time-series analysis. J Korean Med Sci. 2017; 32:999–1008. PMID: 28480659.
Article2. Choi SY, Lee SY, Chi BH, Kim JW, Kim TH, Chang IH. Urbanization may affect the incidence of urolithiasis in South Korea. Springerplus. 2016; 5:1891. PMID: 27843748.
Article3. Chung JD, Kim TH, Myung SC, Moon YT, Kim KD, Chang IH. Influence of overweight on 24-hour urine chemistry studies and recurrent urolithiasis in children. Korean J Urol. 2012; 53:268–274. PMID: 22536471.
Article4. Kim SC, Moon YT, Hong YP, Hwang TK, Choi SH, Kim KJ, et al. Prevalence and risk factors of urinary stones in Koreans. J Korean Med Sci. 1998; 13:138–146. PMID: 9610613.
Article5. Boulay I, Holtz P, Foley WD, White B, Begun FP. Ureteral calculi: diagnostic efficacy of helical CT and implications for treatment of patients. AJR Am J Roentgenol. 1999; 172:1485–1490. PMID: 10350277.
Article6. Fulgham PF, Assimos DG, Pearle MS, Preminger GM. Clinical effectiveness protocols for imaging in the management of ureteral calculous disease: AUA technology assessment. J Urol. 2013; 189:1203–1213. PMID: 23085059.
Article7. Lee DH, Chang IH, Kim JW, Chi BH, Park SB. Usefulness of nonenhanced computed tomography for diagnosing urolithiasis without pyuria in the emergency department. Biomed Res Int. 2015; 2015:810971. PMID: 26421303.
Article8. Ahn S. LOCAT group. LOCAT (low-dose computed tomography for appendicitis trial) comparing clinical outcomes following low- vs standard-dose computed tomography as the first-line imaging test in adolescents and young adults with suspected acute appendicitis: study protocol for a randomized controlled trial. Trials. 2014; 15:28. PMID: 24438500.
Article9. Ibrahim M, Parmar H, Christodoulou E, Mukherji S. Raise the bar and lower the dose: current and future strategies for radiation dose reduction in head and neck imaging. AJNR Am J Neuroradiol. 2014; 35:619–624. PMID: 23449649.
Article10. Kwon JK, Chang IH, Moon YT, Lee JB, Park HJ, Park SB. Usefulness of low-dose nonenhanced computed tomography with iterative reconstruction for evaluation of urolithiasis: diagnostic performance and agreement between the urologist and the radiologist. Urology. 2015; 85:531–538. PMID: 25733262.
Article11. Choi SY, Ahn SH, Choi JD, Kim JH, Lee BI, Kim JI, et al. Determination of optimal imaging settings for urolithiasis CT using filtered back projection (FBP), statistical iterative reconstruction (IR) and knowledge-based iterative model reconstruction (IMR): a physical human phantom study. Br J Radiol. 2016; 89:20150527. PMID: 26577542.
Article12. Park SH, Kim KD, Moon YT, Myung SC, Kim TH, Chang IH, et al. Pilot study of low-dose nonenhanced computed tomography with iterative reconstruction for diagnosis of urinary stones. Korean J Urol. 2014; 55:581–586. PMID: 25237459.
Article13. Malkawi IM, Han E, Atalla CS, Santucci RA, O'Neil B, Wynberg JB. Low-dose (10%) computed tomography may be inferior to standard-dose CT in the evaluation of acute renal colic in the emergency room setting. J Endourol. 2016; 30:493–496. PMID: 26728321.
Article14. Park SB, Kim YS, Lee JB, Park HJ. Knowledge-based iterative model reconstruction (IMR) algorithm in ultralow-dose CT for evaluation of urolithiasis: evaluation of radiation dose reduction, image quality, and diagnostic performance. Abdom Imaging. 2015; 40:3137–3146. PMID: 26197735.
Article15. Guest AR, Cohan RH, Korobkin M, Platt JF, Bundschu CC, Francis IR, et al. Assessment of the clinical utility of the rim and comet-tail signs in differentiating ureteral stones from phleboliths. AJR Am J Roentgenol. 2001; 177:1285–1291. PMID: 11717067.
Article16. Bell TV, Fenlon HM, Davison BD, Ahari HK, Hussain S. Unenhanced helical CT criteria to differentiate distal ureteral calculi from pelvic phleboliths. Radiology. 1998; 207:363–367. PMID: 9577482.
Article17. Heneghan JP, Dalrymple NC, Verga M, Rosenfield AT, Smith RC. Soft-tissue “rim” sign in the diagnosis of ureteral calculi with use of unenhanced helical CT. Radiology. 1997; 202:709–711. PMID: 9051021.
Article18. Boridy IC, Nikolaidis P, Kawashima A, Goldman SM, Sandler CM. Ureterolithiasis: value of the tail sign in differentiating phleboliths from ureteral calculi at nonenhanced helical CT. Radiology. 1999; 211:619–621. PMID: 10352582.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pilot Study of Low-Dose Nonenhanced Computed Tomography With Iterative Reconstruction for Diagnosis of Urinary Stones
- Dosimetric Effects of Low Dose 4D CT Using a Commercial Iterative Reconstruction on Dose Calculation in Radiation Treatment Planning: A Phantom Study
- Diameter of the Solid Component in Subsolid Nodules on Low-Dose Unenhanced Chest Computed Tomography: Measurement Accuracy for the Prediction of Invasive Component in Lung Adenocarcinoma
- Clinical Experience for Radiolucent Stones; A Report of 27 Cases
- Effects of Iterative Reconstruction Algorithm, Automatic Exposure Control on Image Quality, and Radiation Dose: Phantom Experiments with Coronary CT Angiography Protocols
