J Cardiovasc Ultrasound.
2018 Mar;26(1):43-44. 10.4250/jcu.2018.26.1.43.
A Rare Case of Left Ventricular Noncompaction in LEOPARD Syndrome
- Affiliations
-
- 1Department of Internal Medicine, Gyeonsang National University School of Medicine, Gyeongsang National University Hospital, Jinju, Korea. jyhwang@gnu.ac.kr
- KMID: 2407681
- DOI: http://doi.org/10.4250/jcu.2018.26.1.43
Abstract
- No abstract available.
Figure
-
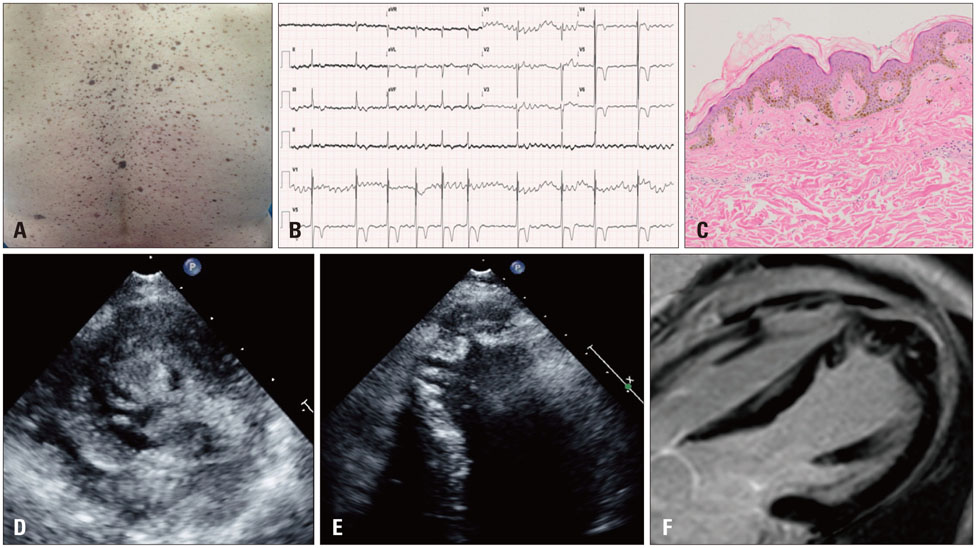
Fig. 1 LEOPARD syndrome clinical presentation. A: Numerous black-brown macules (lentigo) with clearly defined edge over back. B: ECG showed atrial fibrillation and left ventricular strain pattern. C: Microscopic examination showed lots of melanocytes without atypia were concentrated in the deep epidermis layer and the number of melanocytes was markedly elevated (H&E staining, × 200). D: In the parasternal short axis view, the ratio of noncompact/compact layers > 2. E: Apical four chambers view. F: Cardiac MRI revealed that multiple trabeculations in the apical segments. There were no evidences of delayed gadolinium enhancement.
Reference
-
1. Voron DA, Hatfield HH, Kalkhoff RK. Multiple lentigines syndrome. Case report and review of the literature. Am J Med. 1976; 60:447–456.2. Martínez-Quintana E, Rodríguez-González F. LEOPARD syndrome: clinical features and gene mutations. Mol Syndromol. 2012; 3:145–157.
Article3. Limongelli G, Pacileo G, Marino B, Digilio MC, Sarkozy A, Elliott P, Versacci P, Calabro P, De Zorzi A, Di Salvo G, Syrris P, Patton M, McKenna WJ, Dallapiccola B, Calabro R. Prevalence and clinical significance of cardiovascular abnormalities in patients with the LEOPARD syndrome. Am J Cardiol. 2007; 100:736–741.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Noncompaction of Ventricular Myocardium Involving the Right Ventricle
- A case of isolated noncompaction of the ventricular myocardium in an elderly patient
- Stroke in a Young Individual with Left Ventricular Noncompaction and Left Atrium Standstill
- Anesthetic experience of patient with isolated left ventricular noncompaction: a case report
- The Management of Cardiovascular Abnormalities in Patient With LEOPARD Syndrome
