Endocrinol Metab.
2015 Sep;30(3):408-413. 10.3803/EnM.2015.30.3.408.
Untreated Congenital Adrenal Hyperplasia with 17-alpha Hydroxylase/17,20-Lyase Deficiency Presenting as Massive Adrenocortical Tumor
- Affiliations
-
- 1Department of Internal Medicine, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. YUMIE@yuhs.ac
- KMID: 2407094
- DOI: http://doi.org/10.3803/EnM.2015.30.3.408
Abstract
- Congenital adrenal hyperplasia (CAH) with 17alpha-hydroxylase/17,20-lyase deficiency is usually characterized by hypertension and primary amenorrhea, sexual infantilism in women, and pseudohermaphroditism in men. hypertension, and sexual infantilism in women and pseudohermaphroditism in men. In rare cases, a huge adrenal gland tumor can present as a clinical manifestation in untreated CAH. Adrenal cortical adenoma is an even more rare phenotype in CAH with 17alpha-hydroxylase/17,20-lyase deficiency. A 36-year-old female presented with hypertension and abdominal pain caused by a huge adrenal mass. Due to mass size and symptoms, left adrenalectomy was performed. After adrenalectomy, blood pressure remained high. Based on hormonal and genetic evaluation, the patient was diagnosed as CAH with 17alpha-hydroxylase/17,20-lyase deficiency. The possibility of a tumorous change in the adrenal gland due to untreated CAH should be considered. It is important that untreated CAH not be misdiagnosed as primary adrenal tumor as these conditions require different treatments. Adequate suppression of adrenocorticotropic hormone (ACTH) in CAH is also important to treat and to prevent the tumorous changes in the adrenal gland. Herein, we report a case of untreated CAH with 17alpha-hydroxylase/17,20-lyase deficiency presenting with large adrenal cortical adenoma and discuss the progression of adrenal gland hyperplasia due to inappropriate suppression of ACTH secretion.
MeSH Terms
Figure
-
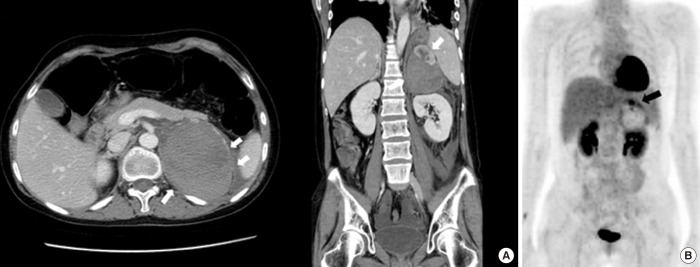
Fig. 1 (A) Computed tomography (CT) scan of the large, 7.6-cm, hemorrhagic mass in the left adrenal gland (white arrows). (B) Fluorodeoxyglucose (FDG) uptake (black arrow) in the solid portion of the mass in 18F-FDG-positron emission tomography-CT.

Fig. 2 Gross finding of adrenal cortical adenoma with degenerative cystic change.

Fig. 3 Computed tomography scan of the right adrenal gland after adrenalectomy (white arrows). (A) Hyperplasia in right adrenal gland immediately after left adrenalectomy. (B) Progression of hyperplasia in right adrenal gland after 3-year follow-up due to poor compliance.
Reference
-
1. Speiser PW, White PC. Congenital adrenal hyperplasia. N Engl J Med. 2003; 349:776–788. PMID: 12930931.
Article2. Bao X, Ding H, Xu Y, Cui G, He Y, Yu X, et al. Prevalence of common mutations in the CYP17A1 gene in Chinese Han population. Clin Chim Acta. 2011; 412:1240–1243. PMID: 21420394.3. van Seters AP, van Aalderen W, Moolenaar AJ, Gorsiro MC, van Roon F, Backer ET. Adrenocortical tumour in untreated congenital adrenocortical hyperplasia associated with inadequate ACTH suppressibility. Clin Endocrinol (Oxf). 1981; 14:325–334. PMID: 6266701.4. Falke TH, van Seters AP, Schaberg A, Moolenaar AJ. Computed tomography in untreated adults with virilizing congenital adrenal cortical hyperplasia. Clin Radiol. 1986; 37:155–160. PMID: 3698500.5. Ravichandran R, Lafferty F, McGinniss MJ, Taylor HC. Congenital adrenal hyperplasia presenting as massive adrenal incidentalomas in the sixth decade of life: report of two patients with 21-hydroxylase deficiency. J Clin Endocrinol Metab. 1996; 81:1776–1779. PMID: 8626833.
Article6. Harinarayana CV, Renu G, Ammini AC, Khurana ML, Ved P, Karmarkar MG, et al. Computed tomography in untreated congenital adrenal hyperplasia. Pediatr Radiol. 1991; 21:103–105. PMID: 2027706.
Article7. Shimshi M, Ross F, Goodman A, Gabrilove JL. Virilizing adrenocortical tumor superimposed on congenital adrenocortical hyperplasia. Am J Med. 1992; 93:338–342. PMID: 1524088.
Article8. Hamwi GJ, Serbin RA, Kruger FA. Does adrenocortical hyperplasia result in adrenocortical carcinoma. N Engl J Med. 1957; 257:1153–1157. PMID: 13493697.
Article9. Daeschner GL. Adrenal cortical adenoma arising in a girl with congenital adrenogenital syndrome. Pediatrics. 1965; 36:141–142. PMID: 14313359.
Article10. Kacem M, Said M, Achour L, Hadj Youssef F, Ben Kacem S, Mahjoub S, et al. Large bilateral adrenal incidentalomas complicating untreated 11B hydroxylase deficiency in the third decade of life. A case report. Ann Endocrinol (Paris). 2000; 61:418–421. PMID: 11084392.11. Chevalier N, Carrier P, Piche M, Chevallier A, Wagner K, Tardy V, et al. Adrenocortical incidentaloma with uncertain prognosis associated with an inadequately treated congenital adrenal hyperplasia. Ann Endocrinol (Paris). 2010; 71:56–59. PMID: 19942208.
Article12. Jaresch S, Kornely E, Kley HK, Schlaghecke R. Adrenal incidentaloma and patients with homozygous or heterozygous congenital adrenal hyperplasia. J Clin Endocrinol Metab. 1992; 74:685–689. PMID: 1311000.
Article13. Mermejo LM, Elias Junior J, Saggioro FP, Tucci Junior S, Castro M, Moreira AC, et al. Giant adrenal myelolipoma associated with 21-hydroxylase deficiency: unusual association mimicking an androgen-secreting adrenocortical carcinoma. Arq Bras Endocrinol Metabol. 2010; 54:419–424. PMID: 20625655.
Article14. Biglieri EG, Herron MA, Brust N. 17-Hydroxylation deficiency in man. J Clin Invest. 1966; 45:1946–1954. PMID: 4288776.
Article15. Tian Q, Yao F, Zhang Y, Tseng H, Lang J. Molecular study of five Chinese patients with 46XX partial 17a-hydroxylase/17,20-lyase deficiency. Gynecol Endocrinol. 2012; 28:234–238. PMID: 21846181.
Article16. Qiao J, Hu RM, Peng YD, Song HD, Peng YW, Gao GF, et al. A complex heterozygous mutation of His373Leu and Asp487-Ser488-Phe489 deletion in human cytochrome P450c17 causes 17alpha-hydroxylase/17,20-lyase deficiency in three Chinese sisters. Mol Cell Endocrinol. 2003; 201:189–195. PMID: 12706306.17. Krone N, Arlt W. Genetics of congenital adrenal hyperplasia. Best Pract Res Clin Endocrinol Metab. 2009; 23:181–192. PMID: 19500762.
Article18. Kim YM, Kang M, Choi JH, Lee BH, Kim GH, Ohn JH, et al. A review of the literature on common CYP17A1 mutations in adults with 17-hydroxylase/17,20-lyase deficiency, a case series of such mutations among Koreans and functional characteristics of a novel mutation. Metabolism. 2014; 63:42–49. PMID: 24140098.19. Yamakita N, Murase H, Yasuda K, Noritake N, Mercado-Asis LB, Miura K. Possible hyperaldosteronism and discrepancy in enzyme activity deficiency in adrenal and gonadal glands in Japanese patients with 17 alpha-hydroxylase deficiency. Endocrinol Jpn. 1989; 36:515–536. PMID: 2555148.
Article20. Cottrell DA, Bello FA, Falko JM. 17 Alpha-hydroxylase deficiency masquerading as primary hyperaldosteronism. Am J Med Sci. 1990; 300:380–382. PMID: 2264576.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of adrenocortical adenoma following long-term treatment in a patient with congenital adrenal hyperplasia
- Two cases of 17α-hydroxylase/17,20-lyase deficiency caused by the CYP17A1 mutation
- Six Cases of Congenital Adrenal Hyperplasia That Were Due to 17alpha-hydroxylase/17,20-lyase Deficiency
- A Case of Adrenocortical Tumor in a 16-Month-Old Boy Presenting with Virilization
- A Case of Congenital Adrenal Hyperlasia Misdiagnosed as Leydig Cell Tumor
