Anesth Pain Med.
2017 Oct;12(4):398-401. 10.17085/apm.2017.12.4.398.
Quadriplegia as a position-related complication after parotidectomy: the need for cooperation between anesthesiologists and surgeons when positioning patients: A case report
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea. aneshmlee@gmail.com
- KMID: 2405862
- DOI: http://doi.org/10.17085/apm.2017.12.4.398
Abstract
- During surgery, the patient is positioned optimally according to the type of operation. Careful attention is required because damage associated with patient positioning may occur during the course of the surgery. Here, we present a case of hyperextension neck injury observed following parotidectomy. A 68-year-old man who was diagnosed with a parotid tumor underwent an elective right partial superficial parotidectomy. After surgery, the patient was not able to move his upper and lower extremities and experienced voiding difficulty. Cervical magnetic resonance imaging showed spinal cord injury at the C3-4 and C5-6 levels. High-dose steroid treatment was started, and emergency laminoplasty C4-5 to C5-6 was performed. Following laminoplasty, motor function was almost fully recovered, but proprioception was weak, and voiding difficulty remained a problem. The patient received rehabilitation treatment in the hospital for about 3 months, demonstrating improvement. He was discharged and continued treatment in the outpatient department.
MeSH Terms
Figure
-
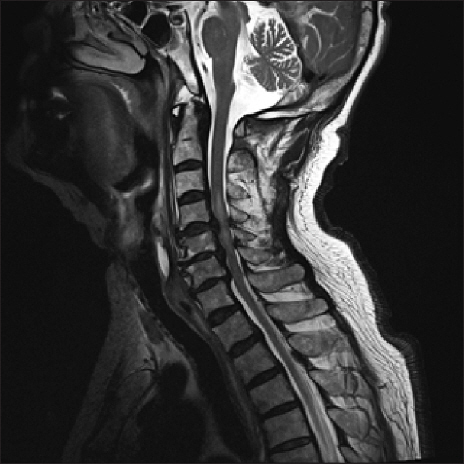
Fig. 1 Sagittal T2-weighted magnetic resonance imaging (MRI) before laminoplasty. Cervical MRI shows broad-based disc extrusion and adjacent ossification of posterior longitudinal ligament at C4-5 and C5-6, and T2 high signal intensity in spinal cord from C3-4 to C5-6.
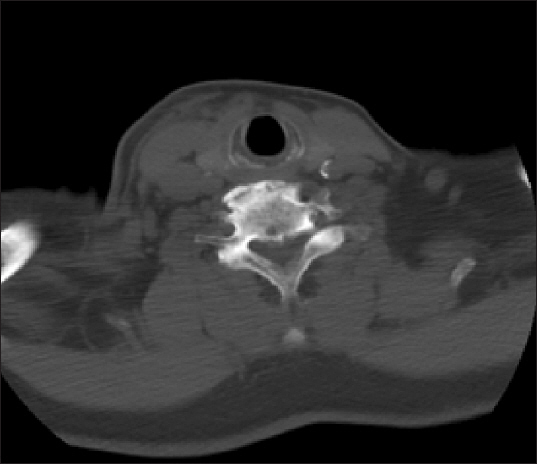
Fig. 2 Neck computed tomography obtained before parotidectomy. Image shows cervical spondylosis and ossification of posterior longitudinal ligament.
Reference
-
1. Compston A. Aids to the investigation of peripheral nerve injuries. Medical Research Council:Nerve Injuries Research Committee. His Majesty's Stationery Office: 1942; pp. 48 (iii) and 74 figures and 7 diagrams; with aids to the examination of the peripheral nervous system. By Michael O’Brien for the Guarantors of Brain. Saunders Elsevier: 2010; pp. [8] 64 and 94 Figures. Brain. 2010; 133:2838–44. DOI: 10.1093/brain/awq270. PMID: 20928945.2. Li CC, Yie JC, Lai CH, Hung MH. Quadriplegia after off-pump coronary artery bypass surgery:look before you place the neck in an extended position. J Cardiothorac Vasc Anesth. 2013; 27:e16–7. DOI: 10.1053/j.jvca.2012.11.012. PMID: 23507022.3. Mercieri M, Paolini S, Mercieri A, De Blasi RA, Palmisani S, Pinto G, et al. Tetraplegia following parathyroidectomy in two long-term haemodialysis patients. Anaesthesia. 2009; 64:1010–3. DOI: 10.1111/j.1365-2044.2009.05944.x. PMID: 19686487.4. Fujioka S, Niimi Y, Hirata K, Nakamura I, Morita S. Tetraplegia after coronary artery bypass grafting. Anesth Analg. 2003; 97:979–80. DOI: 10.1213/01.ANE.0000078585.67412.FE. PMID: 14500143.5. Clancy C, Kolcow W, Scully M, Veerasingam D. Cervical spine stenosis after uneventful coronary artery bypass surgery. J Cardiothorac Vasc Anesth. 2014; 28:e14–5. DOI: 10.1053/j.jvca.2013.10.022. PMID: 24461357.6. Naja Z, Zeidan A, Maaliki H, Zoubeir S, El-Khatib R, Baraka A. Tetraplegia after coronary artery bypass grafting in a patient with undiagnosed cervical stenosis. Anesth Analg. 2005; 101:1883–4. DOI: 10.1213/01.ANE.0000180255.62444.7A. PMID: 16301282.7. Gorur A, Aydemir NA, Yurtseven N, Salih Bilal M. Tetraplegia after coronary artery bypass surgery in a patient with cervical herniation. Innovations (Phila). 2010; 5:134–5. DOI: 10.1097/IMI.0b013e3181d7553b. PMID: 22437364.8. Hwang NC, Singh P, Chua YL. Quadriparesis after cardiac surgery. J Cardiothorac Vasc Anesth. 2008; 22:587–9. DOI: 10.1053/j.jvca.2008.01.022. PMID: 18662638.9. Carron M, Veronese S, Ori C. Tetraplegia following thyroidectomy in a patient with spinal meningioma. Br J Anaesth. 2010; 104:786–7. DOI: 10.1093/bja/aeq106. PMID: 20460575.10. Hirose H, Akhrass R. Tetraplegia after coronary artery bypass, a rare complication. Ann Thorac Cardiovasc Surg. 2005; 11:270–2. PMID: 16148878.11. Agarwal J, Tandon MS, Singh D, Ganjoo P. Quadriplegia in a child following adenotonsillectomy. Anaesthesia. 2013; 68:523–6. DOI: 10.1111/anae.12118. PMID: 23316777.12. Naito M, Ogata K, Nakamoto M, Goya T, Sugioka Y. Destructive spondylo-arthropathy during long-term haemodialysis. J Bone Joint Surg Br. 1992; 74:686–90. PMID: 1527113.13. Gore DR, Sepic SB, Gardner GM. Roentgenographic findings of the cervical spine in asymptomatic people. Spine (Phila Pa 1976). 1986; 11:521–4. DOI: 10.1097/00007632-198607000-00003.14. Boden SD, McCowin PR, Davis DO, Dina TS, Mark AS, Wiesel S. Abnormal magnetic-resonance scans of the cervical spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am. 1990; 72:1178–84. DOI: 10.2106/00004623-199072080-00008. PMID: 2398088.15. Muhle C, Weinert D, Falliner A, Wiskirchen J, Metzner J, Baumer M, et al. Dynamic changes of the spinal canal in patients with cervical spondylosis at flexion and extension using magnetic resonance imaging. Invest Radiol. 1998; 33:444–9. DOI: 10.1097/00004424-199808000-00004. PMID: 9704283.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Quadriplegia after Parotidectomy in a Patient with Asymptomatic Cervical Spondylosis
- Sciatic neuropathy following robot-assisted laparoscopic myomectomy under lithotomy position: A case report
- Patient Positioning in Spine Surgery: What Spine Surgeons Should Know?
- Cooperation with anesthesiologists for acute airway management in the emergency department: A case report
- Conservative Deep Lobe Parotidectomy with Preservation of Superficial Lobe on Pleomorphic Adenoma in Deep Lobe of Parotid: a Case Report
