Predictors of the Frequency of Ethanol Injections for Renal Cyst Ablation: A Preliminary Study
- Affiliations
-
- 1Department of Radiology, Chungbuk National University Hostpital, Cheongju, Korea. sircircle@hanmail.net
- 2Department of Radiology, College of Medicine, Chungbuk National University, Cheongju, Korea.
- KMID: 2405722
- DOI: http://doi.org/10.3348/jksr.2018.78.3.193
Abstract
- PURPOSE
To assess the factors facilitating the prediction of the frequency of ethanol injections in successful renal cyst ablation.
MATERIALS AND METHODS
We retrospectively reviewed the computed tomography and ultrasonography scans of 37 renal cysts. Two radiologists evaluated the characteristics of the presenting renal cysts, including size, calcification, septation, and lobulated configuration. Patients were divided into an "above-four" group and "below-three" group, according to the number of ethanol injections.
RESULTS
Among the 37 renal cysts, six belonged to the "above-four" group and 31 to the "below-three" group. The mean volume of "above-four" group was 409.48 cc and that of the other group was 301.64 cc. Seven renal cysts included three belonging to the "above-four" group, which showed calcification. Twelve renal cysts presented a multilocular appearance with thin septa, and included a cyst classified under the "above-four" group. Three renal cysts had lobulated configuration, with one of them belonging to the "above-four" group.
CONCLUSION
No significant correlation was found among the different factors in the prediction of the frequency of renal cyst ablation. However, calcification was the most useful parameter for prediction of the number of renal cyst ablations needed.
MeSH Terms
Figure
-

Fig. 1. A 55-year-old woman with a Bosniak classification II lesion in the right kidney and she was performed four times ethanol injections. A, B. The renal cyst in the right kidney shows calcification (white arrows) and septa (black arrows) in non-contrast-enhanced (A) and contrast-enhanced (B) axial computed tomography scans. In addition, it has a lobulated margin (white arrowheads) with at least one lobule. C. Like the axial axis view, the coronal axis view shows a lobulated margin (arrowheads) with at least one lobule; since the lobulated margin is visible in two planes, this cyst was classified as a lobulated renal cyst with calcification and thin septa.

Fig. 2. A 57-year-old man with a Bosniak classification I lesion in the left kidney and he was performed two times ethanol injections. A. The contrast-enhanced computed tomography axial scan shows a lobulated margin (arrowheads). B, C. The coronal scan also shows a renal cyst with a lobulated margin (arrowheads) renal cyst; however, this is not accompanied by internal septa or calcification. Hence, this case was classified as a lobulated renal cyst in the left kidney without internal septa or calcification. D. Similarly, a sonogram performed during sclerotherapy also demonstrated a lobulated contour (arrowheads).
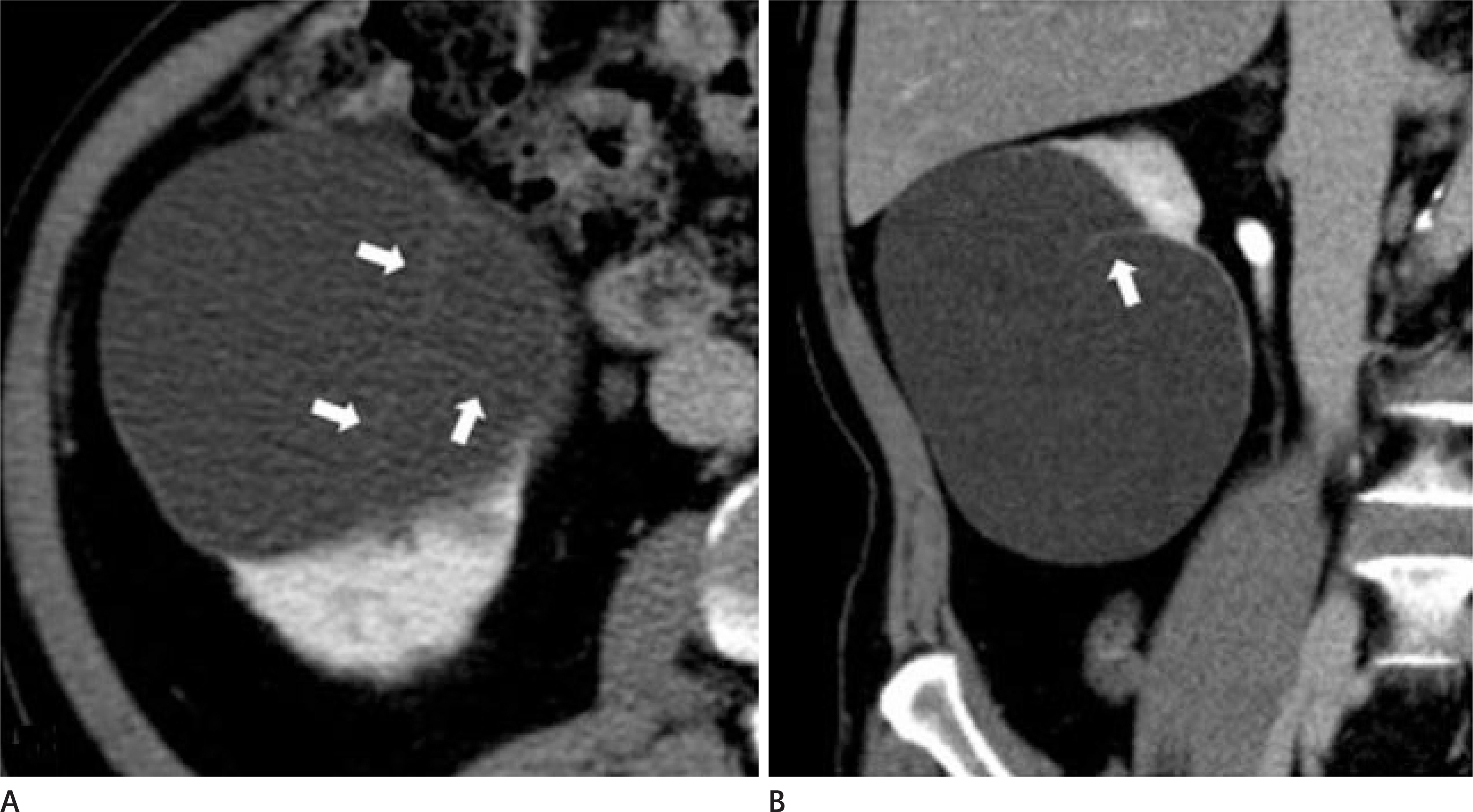
Fig. 3. A 71-year-old man with a Bosniak classification II lesion in the right kidney and he was performed two times ethanol injections. A, B. The axial and coronal contrast-enhanced CT scans show a renal cyst with internal linear density (white arrows). This was classified as a smooth margined renal cyst with thin septa and no calcification.
Reference
-
References
1. Korean Society of Interventional Radiology. Interventional radiology. 2nd ed. Seoul: Ilchokak;2006. p. 681–689.2. Mohsen T, Gomha MA. Treatment of symptomatic simple renal cysts by percutaneous aspiration and ethanol sclerotherapy. BJU Int. 2005; 96:1369–1372.
Article3. Okeke AA, Mitchelmore AE, Keeley FX, Timoney AG. A comparison of aspiration and sclerotherapy with laparoscopic de-roofing in the management of symptomatic simple renal cysts. BJU Int. 2003; 92:610–613.
Article4. el-Diasty TA, Shokeir AA, Tawfeek HA, Mahmoud NA, Nabeeh A, Ghoneim MA. Ethanol sclerotherapy for symptomatic simple renal cysts. J Endourol. 1995; 9:273–276.
Article5. Chung BH, Kim JH, Hong CH, Yang SC, Lee MS. Comparison of single and multiple sessions of percutaneous sclerotherapy for simple renal cyst. BJU Int. 2000; 85:626–627.
Article6. Touloupidis S, Fatles G, Rombis V, Papathanasiou A, Balaxis E. Percutaneous drainage of simple cysts of the kidney: a new method. Urol Int. 2004; 73:169–172.
Article7. Ali TA, Abdelaal MA, Enite A, Badran YA. Ultrasound-guided percutaneous sclerotherapy of simple renal cysts with n-butyl cyanoacrylate and iodized oil mixture as an outpatient procedure. Urol Ann. 2016; 8:51–55.
Article8. Kim SH, Kim SH, Cho JY. Cyst ablation using a mixture of N-butyl cyanoacrylate and iodized oil in patients with autosomal dominant polycystic kidney disease: the longterm results. Korean J Radiol. 2009; 10:377–383.
Article9. Seo TS, Oh JH, Yoon Y, Lim JW, Park SJ, Chang SG, et al. Acetic acid as a sclerosing agent for renal cysts: comparison with ethanol in follow-up results. Cardiovasc Intervent Radiol. 2000; 23:177–181.
Article10. Uemasu J, Fujihara M, Munemura C, Nakamura E, Kawasaki H. Cyst sclerotherapy with minocycline hydrochloride in patients with autosomal dominant polycystic kidney disease. Nephrol Dial Transplant. 1996; 11:843–846.
Article11. Peyromaure M, Debré B, Flam TA. Sclerotherapy of a giant renal cyst with povidone-iodine. J Urol. 2002; 168:2525.
Article12. Kim JH, Lee JT, Kim EK, Won JY, Kim MJ, Lee JD, et al. Percutaneous sclerotherapy of renal cysts with a beta-emitting radionuclide, holmium-166-chitosan complex. Korean J Radiol. 2004; 5:128–133.
Article13. Bean WJ. Renal cysts: treatment with alcohol. Radiology. 1981; 138:329–331.
Article14. Bozkurt FB, Boyvat F, Tekin I, Aytekin C, Coskun M, Ozkardes H. Percutaneous sclerotherapy of a giant benign renal cyst with alcohol. Eur J Radiol. 2001; 40:64–67.
Article15. Lee YR, Lee KB. Ablation of symptomatic cysts using absolute ethanol in 11 patients with autosomal-dominant polycystic kidney disease. Korean J Radiol. 2003; 4:239–242.
Article16. El-Kader OA, Mohyelden K, Metwally AH, Sherif MH, Elnash-er A, Abdelhameed H, et al. Ethanolamine oleate vs. absolute ethanol as sclerosing agents for treating symptomatic simple renal cysts. Arab J Urol. 2014; 12:294–298.
Article17. Demir E, Alan C, Kilciler M, Bedir S. Comparison of ethanol and sodium tetradecyl sulfate in the sclerotherapy of renal cyst. J Endourol. 2007; 21:903–905.
Article18. Egilmez H, Gok V, Oztoprak I, Atalar M, Cetin A, Arslan M, et al. Comparison of CT-guided sclerotherapy with using 95% ethanol and 20% hypertonic saline for managing simple renal cyst. Korean J Radiol. 2007; 8:512–519.
Article19. Omerovic´ S, Zerem E. Alcohol sclerotherapy in the treatment of symptomatic simple renal cysts. Bosn J Basic Med Sci. 2008; 8:337–340.20. Lee SE, Cho JH. The effect of two-injection ethanol sclerotherapy with 5-minute duration of exposure time in simple renal cysts. J Korean Soc Radiol. 2017; 77:113–120.
Article21. Rodriguez-Panadero F, Segado A, Martin Juan J, Ayerbe R, Torres Garcia I, Castillo J. Failure of talc pleurodesis is associated with increased pleural fibrinolysis. Am J Respir Crit Care Med. 1995; 151(3 Pt 1):785–790.
Article22. Genofre EH, Marchi E, Vargas FS. Inflammation and clinical repercussions of pleurodesis induced by intrapleural talc administration. Clinics (Sao Paulo). 2007; 62:627–634.
Article23. Levine E, Grantham JJ. Calcified renal stones and cyst calcifications in autosomal dominant polycystic kidney disease: clinical and CT study in 84 patients. AJR Am J Roentgenol. 1992; 159:77–81.
Article24. Weyman PJ, McClennan BL, Lee JK, Stanley RJ. CT of calcified renal masses. AJR Am J Roentgenol. 1982; 138:1095–1099.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Simple Renal Cyst Treatment: Ultrasound-guided Aspiration Alone or with Instillation of 99% Ethanol into Renal Cyst
- Ultrasound-guided Aspiration and Instillation of 95% Ethanol for Simple Renal Cyst
- Duodenal Stricture due to Necrotizing Pancreatitis following Endoscopic Ultrasound-Guided Ethanol Ablation of a Pancreatic Cyst: A Case Report
- Ultrasound (US)-Guided Ablation of Thyroid Nodules
- Aspiration and Sclerotherapy with 95% Ehtanol for Simple Renal Cyst
