Multimodality Imaging in Patients with Secondary Hypertension: With a Focus on Appropriate Imaging Approaches Depending on the Etiologies
- Affiliations
-
- 1Department of Radiology, Seoul National University Bundang Hospital, Seongnam 13620, Korea. drejchun@hanmail.net
- 2Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam 13620, Korea.
- KMID: 2404924
- DOI: http://doi.org/10.3348/kjr.2018.19.2.272
Abstract
- Although the causes of hypertension are usually unknown, about 10% of the cases occur secondary to specific etiologies, which are often treatable. Common categories of secondary hypertension include renal parenchymal disease, renovascular stenosis, vascular and endocrinologic disorders. For diseases involving the renal parenchyma and adrenal glands, ultrasonography (US), computed tomography (CT) or magnetic resonance (MR) imaging is recommended. For renovascular stenosis and vascular disorders, Doppler US, conventional or noninvasive (CT or MR) angiography is an appropriate modality. Nuclear imaging can be useful in the differential diagnosis of endocrine causes. Radiologists should understand the role of each imaging modality and its typical findings in various causes of secondary hypertension. This article focuses on appropriate imaging approaches in accordance with the categorized etiologies leading to hypertension.
Keyword
MeSH Terms
Figure
-
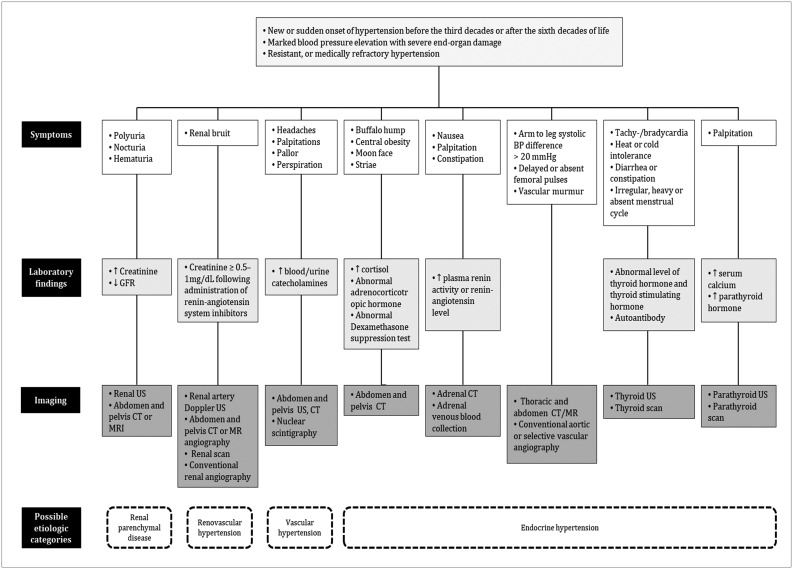
Fig. 1 Appropriate diagnostic imaging approaches consisting of patients' symptoms, laboratory findings, and imaging modalities depending on etiologies of secondary hypertension.BP = blood pressure, CT = computed tomography, GFR = glomerular filtration rate, MR = magnetic resonance, US = ultrasonography,é = elevated, é = decreased
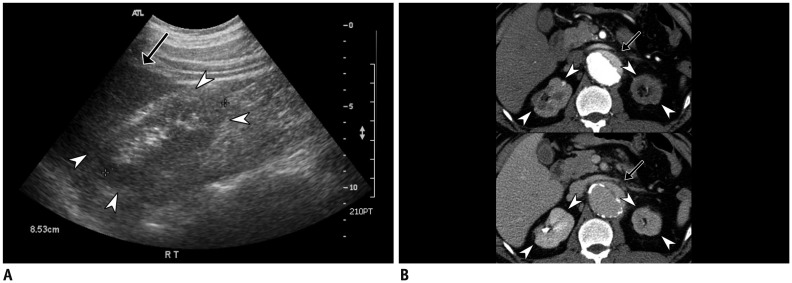
Fig. 2 Glomerulonephritis in 37-year-old male with long history of hypertension and nephrotic range proteinuria.Renal US (A) demonstrates small kidney less than 9 cm in length, with relatively higher parenchymal echogenicity (arrowheads) compared to liver (arrow). CT images (B) from arterial (upper row) and delayed phases (lower row) show irregular contour with atrophic changes in bilateral kidneys (arrowheads). Aortic dissection (arrows), possible complication of long-standing hypertension, is also noted.
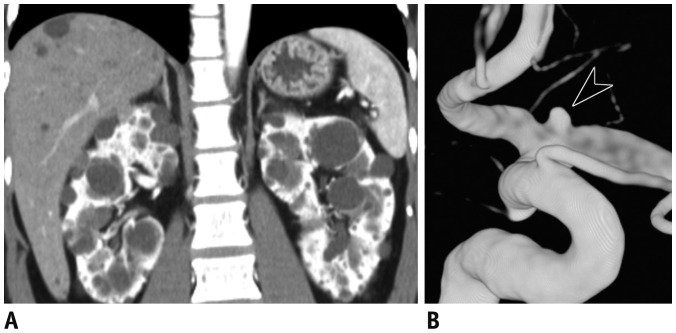
Fig. 3 Autosomal dominant polycystic kidney disease in 37-year-old male with hypertension and family history of hemorrhagic stroke.Coronal CT image (A) shows multiple cysts of variable sizes in bilateral kidneys and liver. Volume-rendered image of left internal carotid artery (B) shows tiny aneurysm (arrowhead) at level of bifurcation.
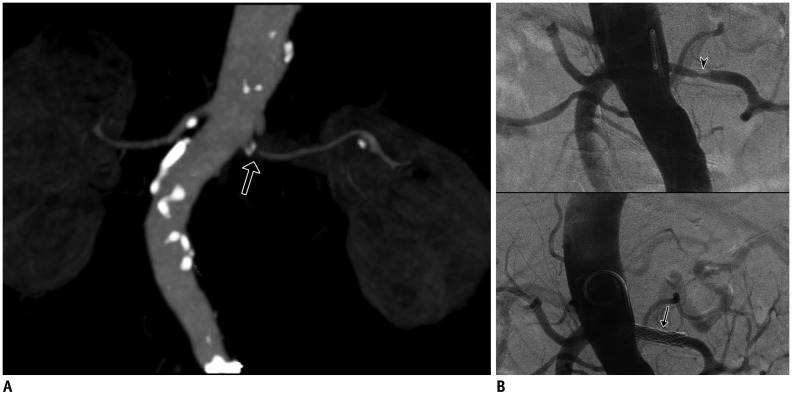
Fig. 4 Atherosclerotic renovascular stenosis in 76-year-old female with hypertension and recent onset azotemia.Coronal CT image with maximum intensity projection (A) shows diffuse atherosclerotic change in aorta and its branches, with focal narrowing (arrow) of proximal segment of left renal artery. Conventional angiography (B) redemonstrated severe stenosis of left renal artery (arrowhead). Lesion was targeted by transluminal angioplasty (arrow), with resultant restoration of luminal diameter. Although blood pressure did not reduce immediately, azotemia was improved.
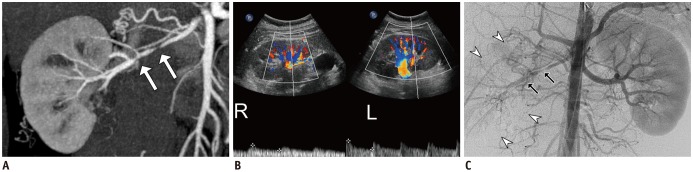
Fig. 5 Fibromuscular dysplasia in 20-year-old male with hypertension.Maximum intensity projection image (A) shows focal narrowing with luminal irregularities in middle segment of right renal artery (arrows). Doppler US (B) reveals tardus-et-parvus waveform with low resistive index of right kidney (labeled as R) compared to left kidney (labeled as L). Aortography and selective right renal arteriography (C) confirmed focal stenosis with luminal irregularities (arrows) in right renal artery causing ipsilateral perfusion delay (arrowheads).
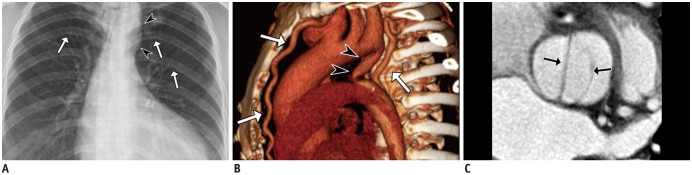
Fig. 6 Coarctation of aorta in 46-year-old female with hypertension and dyspnea on exertion.Plain radiograph of chest (A) shows left ventricular hypertrophy, small contour of aortic arch (arrowheads), and mild notching of a few ribs (arrows). Volume-rendered CT image (B) reveals postductal type of aortic coarctation (arrowheads), with well-developed collaterals via internal mammary and intercostal arteries (arrows). Reformatted image of valve (C) shows bicuspid aortic valve (arrows), one of well-known anomalies associated with coarctation of aorta. Patient underwent corrective surgery (Bentall operation) with subsequent normalization of blood pressure.
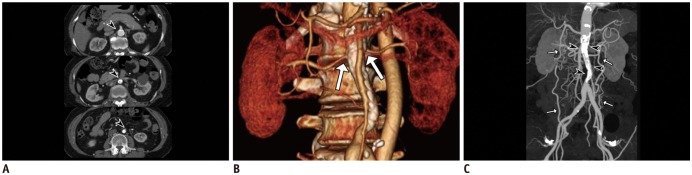
Fig. 7 Mid-aortic dysplastic syndrome in 62-year-old female with hypertension and intermittent claudication.Serial axial CT image (A) shows segmental luminal narrowing of abdominal aorta with calcified vascular wall (arrowheads). Volume-rendered image (B) demonstrates aortic stenosis involving ostia of bilateral renal arteries (arrows). Maximum intensity projection in CT angiography (C) shows segmental narrowing of infrarenal abdominal aorta with concentric calcification (arrowheads), probably due to sequelae of Takayasu aortitis. Note resultant collaterals (arrows) between bilateral intercostal, circumflex iliac, and epigastric arteries.
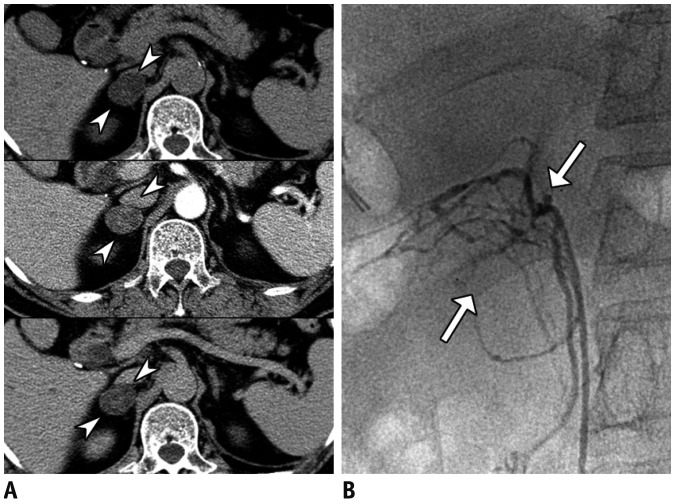
Fig. 8 Primary aldosteronism in 68-year-old male with uncontrolled hypertension, low level of plasma renin activity (0.2 ng/mL/hr) and elevated aldosterone level (47 ng/dL).Incidentally detected right adrenal mass (arrowheads) (A), with attenuation coefficients of 8, 43, and 21 Hounsfield units at pre-contrast (upper column), portal venous (middle column), and delayed phases (lower column), respectively, making absolute percentage washout of 65% and relative percentage washout of 55%, consistent with adenoma. Right adrenal venous sampling (arrows) (B) confirmed high aldosterone level (13680 ng/dL). Subsequent right adrenalectomy yielded lesion that was confirmed to be adenoma.
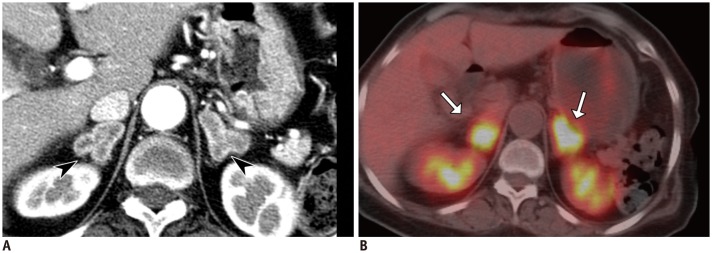
Fig. 9 Cushing's syndrome in 65-year-old female with hypertension, diabetes mellitus, and generalized weakness and markedly elevated adrenocorticotropic hormone (1260 pg/mL).Axial CT scan (A) shows bilateral adrenal masses (arrowheads) with strong cortical enhancement. Whole-body PET (B) shows hypermetabolic adrenal masses (arrows), corresponding to CT. Lesions were surgically resected and were confirmed to be bilateral adrenal cortical hyperplasia.
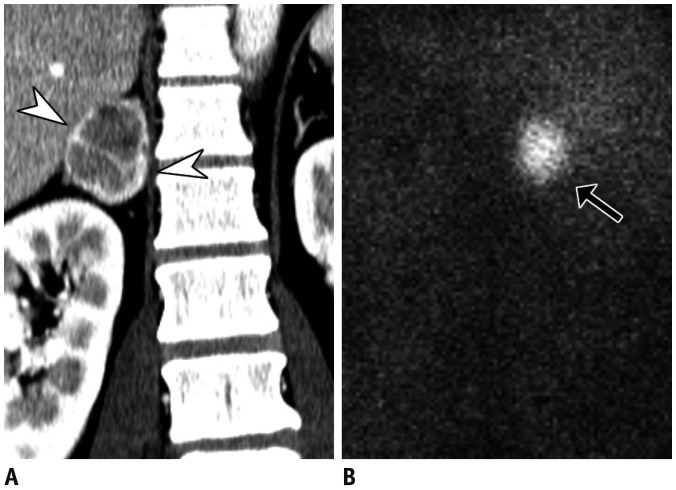
Fig. 10 Pheochromocytoma in 49-year-old male with hypertension, headache, and chest discomfort.Coronal CT image (A) shows heterogeneously enhancing right adrenal mass with lobulated contour (arrowheads). Nuclear scintigraphy (B) shows high uptake of metaiodobenzylguanidine 28 hours after injection (arrow).
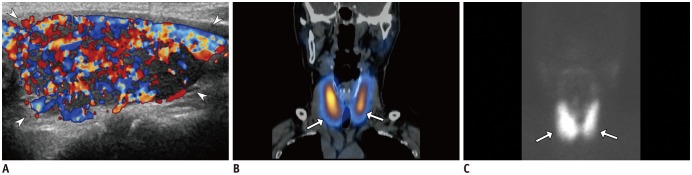
Fig. 11 Thyroid dysfunction in 79-year-old female with hypertension, depressed thyroid-stimulating hormone (< 0.01 µIU/mL), elevated T3 (4.4 ng/mL), and free T4 (> 5.54 ng/dL).Color Doppler US (A) demonstrates diffusely enlarged left thyroid (arrowheads, right not shown) with heterogeneous parenchymal echogenicity, with so-called “thyroid inferno,” appearing as markedly increased vascularity. Coronal image of hybrid single positron emission CT (B) and maximum intensity projection (C) show increased uptake of 99mTc within both thyroid glands (arrows in B and C). Patient was diagnosed with Graves' disease and was started on methimazole.
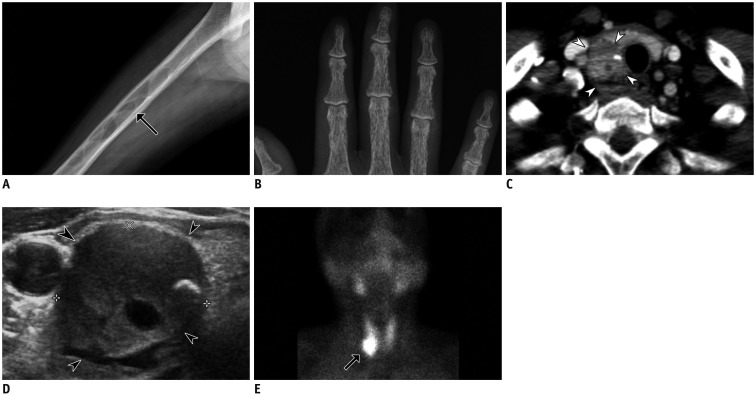
Fig. 12 Hyperparathyroidism in 47-year-old female with hypertension and generalized weakness.Plain radiographs show multiple well-defined osteolytic lesions within femur (arrow) (A), presumably brown tumors, and subperiosteal bone resorption of phalanges of hand (B). Neck CT (C) shows inhomogeneous mass (arrowheads) located inferiorly to right thyroid. US (D) revealed hypoechoic mass in right lower parathyroid (arrowheads) containing focal calcification. Sestamibi scan (E) obtained two hours after radiotracer administration shows high uptake of Tc-99m in right lower neck (arrow). Lesion was later surgically confirmed to be parathyroid adenoma.
Cited by 1 articles
-
Guideline for Cardiovascular Magnetic Resonance Imaging from the Korean Society of Cardiovascular Imaging—Part 1: Standardized Protocol
Yeseul Jo, JeongJae Kim, Chul Hwan Park, Jae Wook Lee, Jee Hye Hur, Dong Hyun Yang, Bae Young Lee, Dong Jin Im, Su Jin Hong, Eun Young Kim, Eun-Ah Park, Pan Ki Kim, Hwan Seok Yong
Korean J Radiol. 2019;20(9):1313-1333. doi: 10.3348/kjr.2019.0398.
Reference
-
1. Sinclair AM, Isles CG, Brown I, Cameron H, Murray GD, Robertson JW. Secondary hypertension in a blood pressure clinic. Arch Intern Med. 1987; 147:1289–1293. PMID: 3606286.
Article2. Anderson GH Jr, Blakeman N, Streeten DH. The effect of age on prevalence of secondary forms of hypertension in 4429 consecutively referred patients. J Hypertens. 1994; 12:609–615. PMID: 7930562.
Article3. Rimoldi SF, Scherrer U, Messerli FH. Secondary arterial hypertension: when, who, and how to screen? Eur Heart J. 2014; 35:1245–1254. PMID: 24366917.
Article4. Shimamoto K, Ando K, Fujita T, Hasebe N, Higaki J, Horiuchi M, et al. The Japanese society of hypertension guidelines for the management of hypertension (JSH 2014). Hypertens Res. 2014; 37:253–390. PMID: 24705419.
Article5. Akpunonu BE, Mulrow PJ, Hoffman EA. Secondary hypertension: evaluation and treatment. Dis Mon. 1996; 42:609–722. PMID: 8948319.
Article6. Chiong JR, Aronow WS, Khan IA, Nair CK, Vijayaraghavan K, Dart RA, et al. Secondary hypertension: current diagnosis and treatment. Int J Cardiol. 2008; 124:6–21. PMID: 17462751.
Article7. Ferguson RK. Cost and yield of the hypertensive evaluation. Experience of a community-based referral clinic. Ann Intern Med. 1975; 82:761–776. PMID: 1138586.8. Danielson M, Dammström B. The prevalence of secondary and curable hypertension. Acta Med Scand. 1981; 209:451–455. PMID: 7257863.
Article9. Kimura G. Clinical pathology and treatment of renin-angiotensin system 2. Chronic kidney disease and the renin-angiotensin system. Intern Med. 2007; 46:1295–1298. PMID: 17704608.
Article10. Usami T, Nakao N, Fukuda M, Takeuchi O, Kamiya Y, Yoshida A, et al. Maps of end-stage renal disease and amounts of angiotensin-converting enzyme inhibitors prescribed in Japan. Kidney Int. 2003; 64:1445–1449. PMID: 12969164.
Article11. Ihm CG. Hypertension in chronic glomerulonephritis. Electrolyte Blood Press. 2015; 13:41–45. PMID: 26848302.
Article12. Joles JA, Koomans HA. Causes and consequences of increased sympathetic activity in renal disease. Hypertension. 2004; 43:699–706. PMID: 14981063.
Article13. Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA task force on practice guidelines (writing committee to develop guidelines for the management of patients with peripheral arterial disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006; 113:e463–e654. PMID: 16549646.
Article14. Nahm AM, Henriquez DE, Ritz E. Renal cystic disease (ADPKD and ARPKD). Nephrol Dial Transplant. 2002; 17:311–314. PMID: 11812890.
Article15. Higashihara E, Aso Y, Shimazaki J, Ito H, Koiso K, Sakai O. Clinical aspects of polycystic kidney disease. J Urol. 1992; 147:329–332. PMID: 1732586.
Article16. Kelleher CL, McFann KK, Johnson AM, Schrier RW. Characteristics of hypertension in young adults with autosomal dominant polycystic kidney disease compared with the general U.S population. Am J Hypertens. 2004; 17(11 Pt 1):1029–1034. PMID: 15533729.
Article17. Wood CG 3rd, Stromberg LJ 3rd, Harmath CB, Horowitz JM, Feng C, Hammond NA, et al. CT and MR imaging for evaluation of cystic renal lesions and diseases. Radiographics. 2015; 35:125–141. PMID: 25590393.
Article18. Pirson Y, Chauveau D, Torres V. Management of cerebral aneurysms in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 2002; 13:269–276. PMID: 11752048.
Article19. Ring T, Spiegelhalter D. Risk of intracranial aneurysm bleeding in autosomal-dominant polycystic kidney disease. Kidney Int. 2007; 72:1400–1402. PMID: 17882153.
Article20. Ong AC. Screening for intracranial aneurysms in ADPKD. BMJ. 2009; 339:b3763. PMID: 19770180.
Article21. Mann SJ, Pickering TG. Detection of renovascular hypertension. State of the art: 1992. Ann Intern Med. 1992; 117:845–853. PMID: 1416561.22. Soulez G, Oliva VL, Turpin S, Lambert R, Nicolet V, Therasse E. Imaging of renovascular hypertension: respective values of renal scintigraphy, renal Doppler US, and MR angiography. Radiographics. 2000; 20:1355–1368. discussion 1368-1372. PMID: 10992024.
Article23. Slovut DP, Olin JW. Fibromuscular dysplasia. N Engl J Med. 2004; 350:1862–1871. PMID: 15115832.
Article24. Olin JW, Sealove BA. Diagnosis, management, and future developments of fibromuscular dysplasia. J Vasc Surg. 2011; 53:826–836.e1. PMID: 21236620.
Article25. Mohammed NM, Mahfouz A, Achkar K, Rafie IM, Hajar R. Contrast-induced nephropathy. Heart Views. 2013; 14:106–116. PMID: 24696755.
Article26. Hellman RN. Gadolinium-induced nephrogenic systemic fibrosis. Semin Nephrol. 2011; 31:310–316. PMID: 21784280.
Article27. Kim HD, Kim MN, Kim SA, Choi SI, Choi JY, Seo JH, et al. Resistant hypertension caused by stenosis of the aorta in elderly women: three case reports. Clin Hypertens. 2014; 20:5. PMID: 26893910.
Article28. Viera AJ, Neutze DM. Diagnosis of secondary hypertension: an age-based approach. Am Fam Physician. 2010; 82:1471–1478. PMID: 21166367.29. Wu MH, Chen HC, Kao FY, Huang SK. Risk of systemic hypertension and cerebrovascular accident in patients with aortic coarctation aged <60 years (from a national database study). Am J Cardiol. 2015; 116:779–784. PMID: 26100586.30. Abbruzzese PA, Aidala E. Aortic coarctation: an overview. J Cardiovasc Med (Hagerstown). 2007; 8:123–128. PMID: 17299295.
Article31. Nance JW, Ringel RE, Fishman EK. Coarctation of the aorta in adolescents and adults: a review of clinical features and CT imaging. J Cardiovasc Comput Tomogr. 2016; 10:1–12. PMID: 26639936.
Article32. Sebastià C, Quiroga S, Boyé R, Perez-Lafuente M, Castellà E, Alvarez-Castells A. Aortic stenosis: spectrum of diseases depicted at multisection CT. Radiographics. 2003; 23(Spec No):S79–S91. PMID: 14557504.
Article33. Ho VB, Bakalov VK, Cooley M, Van PL, Hood MN, Burklow TR, et al. Major vascular anomalies in Turner syndrome: prevalence and magnetic resonance angiographic features. Circulation. 2004; 110:1694–1700. PMID: 15353492.
Article34. Campbell M. Natural history of coarctation of the aorta. Br Heart J. 1970; 32:633–640. PMID: 5470045.
Article35. Connolly JE, Wilson SE, Lawrence PL, Fujitani RM. Middle aortic syndrome: distal thoracic and abdominal coarctation, a disorder with multiple etiologies. J Am Coll Surg. 2002; 194:774–781. PMID: 12081068.36. Delis KT, Gloviczki P. Middle aortic syndrome: from presentation to contemporary open surgical and endovascular treatment. Perspect Vasc Surg Endovasc Ther. 2005; 17:187–203. PMID: 16273154.
Article37. Daghero F, Bueno N, Peirone A, Ochoa J, Torres GF, Ganame J. Coarctation of the abdominal aorta: an uncommon cause of arterial hypertension and stroke. Circ Cardiovasc Imaging. 2008; 1:e4. e6. PMID: 19808505.39. Sica DA. Endocrine causes of secondary hypertension. J Clin Hypertens (Greenwich). 2008; 10:534–540. PMID: 18607139.
Article40. Gallay BJ, Ahmad S, Xu L, Toivola B, Davidson RC. Screening for primary aldosteronism without discontinuing hypertensive medications: plasma aldosterone-renin ratio. Am J Kidney Dis. 2001; 37:699–705. PMID: 11273868.
Article41. Eide IK, Torjesen PA, Drolsum A, Babovic A, Lilledahl NP. Low-renin status in therapy-resistant hypertension: a clue to efficient treatment. J Hypertens. 2004; 22:2217–2226. PMID: 15480108.42. Funder JW, Carey RM, Fardella C, Gomez-Sanchez CE, Mantero F, Stowasser M, et al. Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2008; 93:3266–3281. PMID: 18552288.
Article43. Boland GW, Lee MJ, Gazelle GS, Halpern EF, McNicholas MM, Mueller PR. Characterization of adrenal masses using unenhanced CT: an analysis of the CT literature. AJR Am J Roentgenol. 1998; 171:201–204. PMID: 9648789.
Article44. Sohaib SA, Peppercorn PD, Allan C, Monson JP, Grossman AB, Besser GM, et al. Primary hyperaldosteronism (Conn syndrome): MR imaging findings. Radiology. 2000; 214:527–531. PMID: 10671606.
Article45. Blake MA, Kalra MK, Sweeney AT, Lucey BC, Maher MM, Sahani DV, et al. Distinguishing benign from malignant adrenal masses: multi-detector row CT protocol with 10-minute delay. Radiology. 2006; 238:578–585. PMID: 16371582.
Article46. Korobkin M, Brodeur FJ, Francis IR, Quint LE, Dunnick NR, Londy F. CT time-attenuation washout curves of adrenal adenomas and nonadenomas. AJR Am J Roentgenol. 1998; 170:747–752. PMID: 9490968.
Article47. Peña CS, Boland GW, Hahn PF, Lee MJ, Mueller PR. Characterization of indeterminate (lipid-poor) adrenal masses: use of washout characteristics at contrast-enhanced CT. Radiology. 2000; 217:798–802. PMID: 11110946.
Article48. Seo JM, Park BK, Park SY, Kim CK. Characterization of lipid-poor adrenal adenoma: chemical-shift MRI and washout CT. AJR Am J Roentgenol. 2014; 202:1043–1450. PMID: 24758658.
Article49. Rossi GP, Sacchetto A, Chiesura-Corona M, De Toni R, Gallina M, Feltrin GP, et al. Identification of the etiology of primary aldosteronism with adrenal vein sampling in patients with equivocal computed tomography and magnetic resonance findings: results in 104 consecutive cases. J Clin Endocrinol Metab. 2001; 86:1083–1090. PMID: 11238490.
Article50. Raff H, Sharma ST, Nieman LK. Physiological basis for the etiology, diagnosis, and treatment of adrenal disorders: Cushing's syndrome, adrenal insufficiency, and congenital adrenal hyperplasia. Compr Physiol. 2014; 4:739–769. PMID: 24715566.
Article51. Sohaib SA, Hanson JA, Newell-Price JD, Trainer PJ, Monson JP, Grossman AB, et al. CT appearance of the adrenal glands in adrenocorticotrophic hormone-dependent Cushing's syndrome. AJR Am J Roentgenol. 1999; 172:997–1002. PMID: 10587135.
Article52. Rockall AG, Babar SA, Sohaib SA, Isidori AM, Diaz-Cano S, Monson JP, et al. CT and MR imaging of the adrenal glands in ACTH-independent cushing syndrome. Radiographics. 2004; 24:435–452. PMID: 15026592.
Article53. Sukor N. Endocrine hypertension--current understanding and comprehensive management review. Eur J Intern Med. 2011; 22:433–440. PMID: 21925049.54. Tischler AS. Pheochromocytoma and extra-adrenal paraganglioma: updates. Arch Pathol Lab Med. 2008; 132:1272–1284. PMID: 18684026.
Article55. Leung K, Stamm M, Raja A, Low G. Pheochromocytoma: the range of appearances on ultrasound, CT, MRI, and functional imaging. AJR Am J Roentgenol. 2013; 200:370–378. PMID: 23345359.
Article56. Prisant LM, Gujral JS, Mulloy AL. Hyperthyroidism: a secondary cause of isolated systolic hypertension. J Clin Hypertens (Greenwich). 2006; 8:596–599. PMID: 16896276.
Article57. Marcisz C, Jonderko G, Kucharz EJ. Influence of short-time application of a low sodium diet on blood pressure in patients with hyperthyroidism or hypothyroidism during therapy. Am J Hypertens. 2001; 14:995–1002. PMID: 11710792.
Article58. Nachiappan AC, Metwalli ZA, Hailey BS, Patel RA, Ostrowski ML, Wynne DM. The thyroid: review of imaging features and biopsy techniques with radiologic-pathologic correlation. Radiographics. 2014; 34:276–293. PMID: 24617678.
Article59. Silverberg SJ, Bilezikian JP. The diagnosis and management of asymptomatic primary hyperparathyroidism. Nat Clin Pract Endocrinol Metab. 2006; 2:494–503. PMID: 16957763.
Article60. Feldstein CA, Akopian M, Pietrobelli D, Olivieri A, Garrido D. Long-term effects of parathyroidectomy on hypertension prevalence and circadian blood pressure profile in primary hyperparathyroidism. Clin Exp Hypertens. 2010; 32:154–158. PMID: 20504122.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Assessment of Right Ventricular Function in Pulmonary Hypertension with Multimodality Imaging
- Multi Modality Imaging Features of Cardiac Myxoma
- Multimodality Imaging in Coronary Artery Disease: Focus on Computed Tomography
- FDG-PET in Multimodality Assessment of Cardiac Myxoma
- Aortic Coarctation Following Aortic Valve Replacement: Problem Solving with Multimodality Cardiac Imaging
