Natural History of Untreated Coronary Total Occlusions Revealed with Follow-Up Semi-Automated Quantitative Coronary CT Angiography: The Morphological Characteristics of Initial CT Predict Occlusion Shortening
- Affiliations
-
- 1Institute of Diagnostic and Interventional Radiology, Shanghai Jiao Tong University Affiliated Sixth People's Hospital, Shanghai 200233, China. andrewssmu@msn.com
- 2Department of Cardiology, Shanghai Jiao Tong University Affiliated Sixth People's Hospital, Shanghai 200233, China.
- 3Siemens Healthcare Ltd., Shanghai 201318, China.
- KMID: 2404922
- DOI: http://doi.org/10.3348/kjr.2018.19.2.256
Abstract
OBJECTIVE
To investigate the morphological changes of coronary chronic total occlusion (CTO) as determined by coronary computed tomography angiography (CCTA) follow-up using semi-automated quantitative analysis.
MATERIALS AND METHODS
Thirty patients with 31 CTO lesions confirmed by invasive coronary angiography and baseline/follow-up CCTA were retrospectively included. CTOs were quantitatively analyzed by a semi-automated coronary plaque analysis software (Coronary Plaque Analysis, version 2.0, Siemens) after manually determining the lesion border. Recanalized lumen was defined as the linear-like enhanced opacity traversing the non-opacified occluded segment. Other parameters, such as total occlusion length, total occlusion volume, volume with low attenuation component (< 30 Hounsfield unit [HU]), volume with middle to high attenuation component (30-190 HU) as well as the calcification volume, were also recorded.
RESULTS
Recanalized lumen was found within 48.4% (15/31) occlusions on the follow-up CCTA, compared to 45.2% (14/31) occlusions on the baseline CCTA. Eleven of 14 lesions (78.6%) with CT-visible recanalized lumen within CTOs had a shorter occlusion length on follow-up compared to only 3 of 17 lesions (17.6%) without CT-visible recanalized lumen (odds ratio, 17.1, p < 0.001). The percentage of low attenuation component of occlusions was smaller on follow-up CCTA compared to baseline value (18.1 ± 20.1% vs. 22.6 ± 19.6%, p = 0.033).
CONCLUSION
Coronary computed tomography angiography enables non-invasive characterization of natural progression of untreated CTO lesions. Recanalized lumen within CTOs observed at baseline CCTA was associated with shortening of occlusion length on follow-up. Compared to their earlier stage, occlusions of later stage were presented with higher density of non-calcified components.
Keyword
MeSH Terms
Figure
-
Fig. 1 Flow chart of inclusion and exclusion.AMI = acute myocardial infarction, CCTA = coronary computed tomography angiography, CTO = chronic total occlusion, ICA = invasive coronary angiography
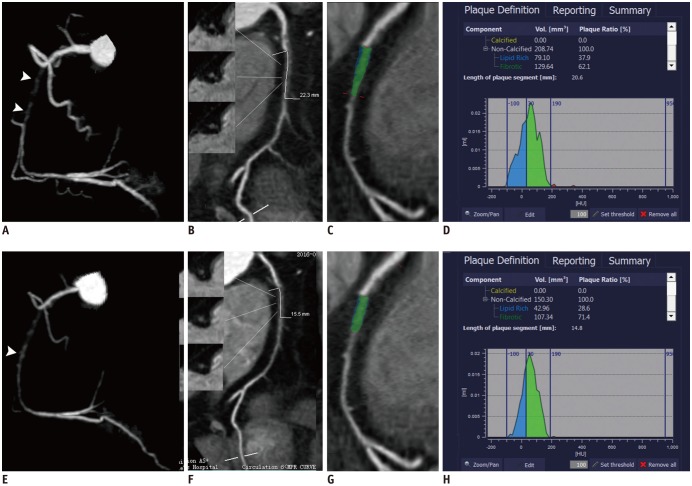
Fig. 2 Representative case of CTO in 65-year-old male patient with baseline (A-D) and follow-up (22 months later) (E-H) CCTA.A. 3D-MIP image showed CTO lesion of middle RCA with visible recanalized lumen (arrowhead) on baseline CCTA. B. Occlusion length measured on CPR image was 22.3 mm. C. Color-coded map revealed components with different CT attenuation within occlusion. D. Histogram demonstrated calculated volume of components with different CT attenuation within occlusion. E. 3D-MIP image showed CTO lesion of middle RCA with shorter occlusion length on follow CCTA. Previously scattered recanalized lumen connected to distal end of occlusion (arrowhead). F. Occlusion length measured on CPR image was 15.5 mm. G. Color-coded map revealed components with different CT attenuation within occlusion. H. Histogram demonstrated decreased volume percentage of component with low CT attenuation within occlusion. CPR = curved planar reformation, CT = computed tomography, MIP = maximum intensity projection, RCA = right coronary artery, 3D = three-dimensional
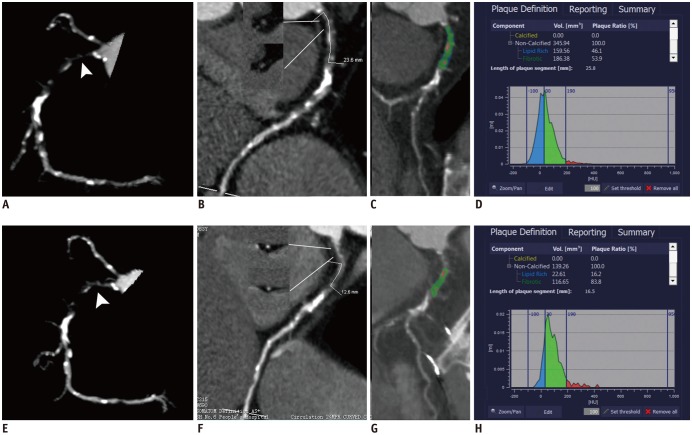
Fig. 3 Representative case of CTO in 62-year-old male patient with baseline (A-D) and follow-up (12 months later) (E-H) CCTA.A. 3D-MIP image showed CTO lesion of proximal RCA with visible recanalized lumen (arrowhead) on baseline CCTA. B. Occlusion length measured on CPR image was 23.6 mm. C. Color-coded map revealed components with different CT attenuation within occlusion. D. Histogram demonstrated calculated volume of components with different CT attenuation within occlusion. E. 3D-MIP image showed CTO lesion of proximal RCA with shorter occlusion length on follow CCTA. Previously scattered recanalized lumen connected to proximal end of occlusion (arrowhead). F. Occlusion length measured on CPR image was 12.6 mm. G. Color-coded map revealed components with different CT attenuation within occlusion. H. Histogram demonstrated decreased volume percentage of component with low CT attenuation within occlusion.
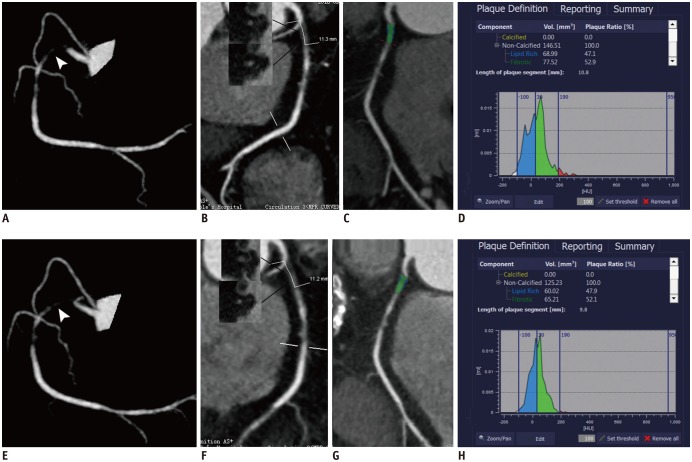
Fig. 4 Representative case of CTO in 58-year-old female patient with baseline (A-D) and follow-up (12 months later) (E-H) CCTA.A. 3D-MIP image showed CTO lesion of proximal RCA with visible recanalized lumen (arrowhead) on baseline CCTA. B. Occlusion length measured on CPR image was 11.3 mm. C. Color-coded map revealed components with different CT attenuation within occlusion. D. Histogram demonstrated calculated volume of components with different CT attenuation within occlusion. E. 3D-MIP image showed CTO lesion of proximal RCA with similar morphology on follow CCTA (arrowhead). F. Occlusion length measured on CPR image was 11.2 mm. G. Color-coded map revealed components with different CT attenuation within occlusion. H. Histogram demonstrated similar volume percentage of component with low CT attenuation within occlusion.
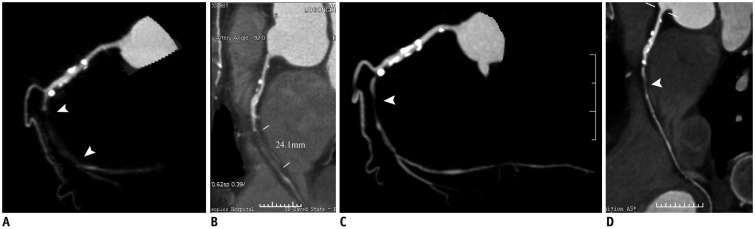
Fig. 5 Representative case of CTO in 73-year-old male patient with baseline (A, B) and follow-up (32 months later) (C, D) CCTA.A. 3D-MIP image showed CTO lesion of middle RCA with visible recanalized lumen (arrowhead) on baseline CCTA. B. Occlusion length measured on CPR image was 24.1 mm. C. 3D-MIP image showed complete spontaneous recanalization of occlusion on follow CCTA (arrowhead). D. CPR image confirmed complete spontaneous recanalization of occlusion with residual stenosis (arrowhead).
Reference
-
1. Stone GW, Kandzari DE, Mehran R, Colombo A, Schwartz RS, Bailey S, et al. Percutaneous recanalization of chronically occluded coronary arteries: a consensus document: part I. Circulation. 2005; 112:2364–2372. PMID: 16216980.2. Suero JA, Marso SP, Jones PG, Laster SB, Huber KC, Giorgi LV, et al. Procedural outcomes and long-term survival among patients undergoing percutaneous coronary intervention of a chronic total occlusion in native coronary arteries: a 20-year experience. J Am Coll Cardiol. 2001; 38:409–414. PMID: 11499731.
Article3. Prasad A, Rihal CS, Lennon RJ, Wiste HJ, Singh M, Holmes DR Jr. Trends in outcomes after percutaneous coronary intervention for chronic total occlusions: a 25-year experience from the Mayo Clinic. J Am Coll Cardiol. 2007; 49:1611–1618. PMID: 17433951.4. Chung CM, Nakamura S, Tanaka K, Tanigawa J, Kitano K, Akiyama T, et al. Effect of recanalization of chronic total occlusions on global and regional left ventricular function in patients with or without previous myocardial infarction. Catheter Cardiovasc Interv. 2003; 60:368–374. PMID: 14571489.
Article5. Olivari Z, Rubartelli P, Piscione F, Ettori F, Fontanelli A, Salemme L, et al. Immediate results and one-year clinical outcome after percutaneous coronary interventions in chronic total occlusions: data from a multicenter, prospective, observational study (TOAST-GISE). J Am Coll Cardiol. 2003; 41:1672–1678. PMID: 12767645.6. Hannan EL, Racz M, Holmes DR, King SB 3rd, Walford G, Ambrose JA, et al. Impact of completeness of percutaneous coronary intervention revascularization on long-term outcomes in the stent era. Circulation. 2006; 113:2406–2412. PMID: 16702469.
Article7. Srivatsa SS, Edwards WD, Boos CM, Grill DE, Sangiorgi GM, Garratt KN, et al. Histologic correlates of angiographic chronic total coronary artery occlusions: influence of occlusion duration on neovascular channel patterns and intimal plaque composition. J Am Coll Cardiol. 1997; 29:955–963. PMID: 9120181.8. Fefer P, Robert N, Qiang B, Liu G, Munce N, Anderson K, et al. Characterisation of a novel porcine coronary artery CTO model. EuroIntervention. 2012; 7:1444–1452. PMID: 22522554.
Article9. Li M, Zhang J, Pan J, Lu Z. Coronary total occlusion lesions: linear intrathrombus enhancement at CT predicts better outcome of percutaneous coronary intervention. Radiology. 2013; 266:443–451. PMID: 23204539.
Article10. Li M, Zhang J, Pan J, Lu Z. Obstructive coronary artery disease: reverse attenuation gradient sign at CT indicates distal retrograde flow--a useful sign for differentiating chronic total occlusion from subtotal occlusion. Radiology. 2013; 266:766–772. PMID: 23220898.
Article11. Zhang J, Li Y, Li M, Pan J, Lu Z. Collateral vessel opacification with CT in patients with coronary total occlusion and its relationship with downstream myocardial infarction. Radiology. 2014; 271:703–710. PMID: 24555634.
Article12. Li Y, Xu N, Zhang J, Li M, Lu Z, Wei M, et al. Procedural success of CTO recanalization: comparison of the J-CTO score determined by coronary CT angiography to invasive angiography. J Cardiovasc Comput Tomogr. 2015; 9:578–584. PMID: 26232276.
Article13. Li M, Liu S, Zhang J, Lu Z, Wei M, Chun EJ, et al. Coronary competitive reverse flow: imaging findings at CT angiography and correlation with invasive coronary angiography. J Cardiovasc Comput Tomogr. 2015; 9:202–208. PMID: 25843241.
Article14. Zhang J, Xu N, Li Y, Li M, Lu Z, Wei M. Evaluation of collateral channel classification by computed tomography: the feasibility study with reference to invasive coronary angiography. Int J Cardiovasc Imaging. 2015; 31:1643–1650. PMID: 26288955.
Article15. Yu M, Xu N, Zhang J, Li Y, Li M, Lu Z, et al. CT features in the early and late stages of chronic total coronary occlusions. J Cardiovasc Comput Tomogr. 2015; 9:572–577. PMID: 26255169.
Article16. Katsuragawa M, Fujiwara H, Miyamae M, Sasayama S. Histologic studies in percutaneous transluminal coronary angioplasty for chronic total occlusion: comparison of tapering and abrupt types of occlusion and short and long occluded segments. J Am Coll Cardiol. 1993; 21:604–611. PMID: 8436741.
Article17. Morino Y, Abe M, Morimoto T, Kimura T, Hayashi Y, Muramatsu T, et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011; 4:213–221. PMID: 21349461.18. Munce NR, Strauss BH, Qi X, Weisbrod MJ, Anderson KJ, Leung G, et al. Intravascular and extravascular microvessel formation in chronic total occlusions a micro-CT imaging study. JACC Cardiovasc Imaging. 2010; 3:797–805. PMID: 20705258.19. Hoebers LP, Claessen BE, Dangas GD, Råmunddal T, Mehran R, Henriques JP. Contemporary overview and clinical perspectives of chronic total occlusions. Nat Rev Cardiol. 2014; 11:458–469. PMID: 24866424.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Changes in Coronary Perfusion after Occlusion of Coronary Arteries in Kawasaki Disease
- Noninvasive Detection of Coronary Atherosclerotic Plaques and Assessment of Stenosis Degree at Multidetector CT Coronary Angiography
- Role of Coronary CT Angiography in Coronary Revascularization
- Percutaneous Transluminal Coronary Angioplasty in Total Coronary Artery Occlusion
- Determination of Early Graft Patency Using CT Angiography after Coronary Artery Bypass Surgery
