Comparison of the Efficacy and Prognostic Factors of Transarterial Chemoembolization Plus Microwave Ablation versus Transarterial Chemoembolization Alone in Patients with a Large Solitary or Multinodular Hepatocellular Carcinomas
- Affiliations
-
- 1Department of Minimal-Invasive Intervention, The Affiliated Cancer Hospital of Zhengzhou University, Zhengzhou 450008, China.
- 2Department of Medical Gastroenterology, The Affiliated Cancer Hospital of Zhengzhou University, Zhengzhou 450008, China. zlnklsx@163.com
- KMID: 2404920
- DOI: http://doi.org/10.3348/kjr.2018.19.2.237
Abstract
OBJECTIVE
To evaluate the efficacy and prognostic factors associated with transcatheter arterial chemoembolization (TACE) combined with microwave ablation (MWA) versus TACE alone for a large solitary or multinodular hepatocellular carcinomas (HCCs).
MATERIALS AND METHODS
This retrospective study involved 258 patients with a large solitary or multinodular HCCs (not more than 10 tumors) who underwent TACE + MWA (n = 92) or TACE alone (n = 166) between July 2011 and April 2015. Local tumor control, survival outcomes, and complications were compared between the two groups. Prognostic factors for time to progression (TTP) and overall survival (OS) were evaluated by univariate and multivariate analyses.
RESULTS
The median duration of follow-up was 21.2 months (range, 4-45 months). The median TTP and OS were 12.5 months and 26.6 months, respectively, for the TACE + MWA group and 6.7 months and 17.1 months, respectively, for the TACE group (p < 0.001). The 1-, 2-, and 3-year OS rates were 85.9, 59.8, and 32.6%, respectively, for the TACE + MWA group and 59.0, 40.4, and 11.4%, respectively, for the TACE group (p < 0.001). The corresponding recurrence rates were 47.8, 78.3, and 94.6% for the TACE + MWA group, respectively, and 74.7, 96.4, and 97.6%, respectively, for the TACE group (p < 0.001). Logistic regression analyses showed that the treatment method, tumor size, and tumor number were significant prognostic factors for TTP and OS.
CONCLUSION
TACE + MWA appears to have more advantages compared to TACE in prolonging OS, with a satisfactory TTP, for inpatients with solitary large or multinodular HCCs. Treatment method, tumor size, and tumor number are significant prognostic factors for TTP and OS. Further randomized, multi-center, prospective trials are required to confirm the findings of this study.
Keyword
MeSH Terms
Figure
-
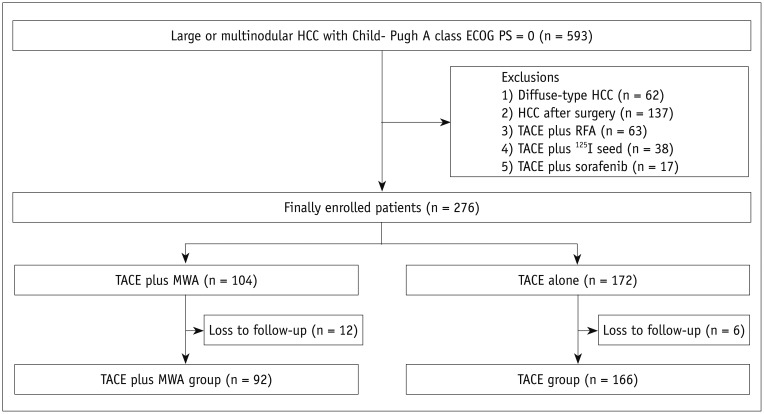
Fig. 1 Study flow chart showing selection of 258 patients who were finally included in study.Flow diagram of progress of 258 patients through enrolment, allocation, follow-up and data analysis phases of our study. ECOG PS = Eastern Cooperative Oncology Group Performance Status, HCC = hepatocellular carcinoma, MWA = microwave ablation, RFA = radiofrequency ablation, TACE = transcatheter arterial chemoembolization

Fig. 2 57-year-old man with multinodular HCC who underwent TACE + MWA combination treatment.A. Non-enhanced CT imaging revealed lipiodol deposits in multinodular HCC (arrowheads). B. CT image during MWA procedure showing antenna has reached opposite edge of tumor via its center (arrowheads). C. Contrast-enhanced MRI image (6 months post-ablation therapy) showing homogeneous hypointense non-enhancing areas (ablation beds, arrowheads) without residual enhancement, denoting successful ablation and complete response.
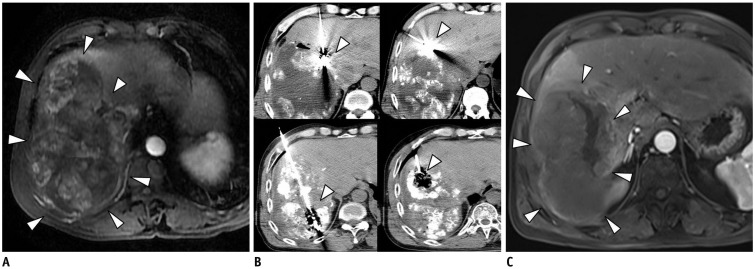
Fig. 3 58-year-old man with HCC who underwent CT-guided MWA after TACE.A. Diagnosis of HCC was based on findings on contrast-enhanced MRI and high AFP concentration (563 ng/mL). Lesion measures 13 cm in longest diameter (arrowheads). B. After TACE procedure, CT-guided MWA was performed to control residual tumor in target lesion (arrowheads). Patient underwent TACE + MWA combination therapy twice. C. Contrast-enhanced MRI scan 6 months after combination treatment showing non-enhancing thermal scar (arrowheads) at site of original tumor and no intrahepatic recurrence. AFP = alpha-fetoprotein
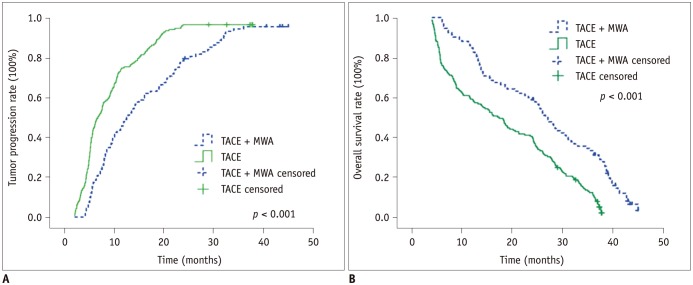
Fig. 4 Tumor progression rate (A) and overall survival rate (B) of patients in TACE + MWA and TACE alone groups.
Cited by 1 articles
-
Comparison of Combined Therapy Using Conventional Chemoembolization and Radiofrequency Ablation Versus Conventional Chemoembolization for Ultrasound-Invisible Early-Stage Hepatocellular Carcinoma (Barcelona Clinic Liver Cancer Stage 0 or A)
Hyukjoon Lee, Chang Jin Yoon, Nak Jong Seong, Sook-Hyang Jeong, Jin-Wook Kim
Korean J Radiol. 2018;19(6):1130-1139. doi: 10.3348/kjr.2018.19.6.1130.
Reference
-
1. Kishore S, Friedman T, Madoff DC. Update on embolization therapies for hepatocellular carcinoma. Curr Oncol Rep. 2017; 19:40. PMID: 28421483.
Article2. Jung YK, Jung CH, Seo YS, Kim JH, Kim TH, Yoo YJ, et al. BCLC stage B is a better designation for single large hepatocellular carcinoma than BCLC stage A. J Gastroenterol Hepatol. 2016; 31:467–474. PMID: 26332049.
Article3. Llovet JM, Di Bisceglie AM, Bruix J, Kramer BS, Lencioni R, Zhu AX, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. J Natl Cancer Inst. 2008; 100:698–711. PMID: 18477802.
Article4. Wáng YX, De Baere T, Idée JM, Ballet S. Transcatheter embolization therapy in liver cancer: an update of clinical evidences. Chin J Cancer Res. 2015; 27:96–121. PMID: 25937772.5. Lencioni R. Chemoembolization for hepatocellular carcinoma. Semin Oncol. 2012; 39:503–509. PMID: 22846867.
Article6. Farinati F, Giacomin A, Vanin V, Giannini E, Trevisani F. TACE treatment in hepatocellular carcinoma: what should we do now? J Hepatol. 2012; 57:221–222. PMID: 22286000.
Article7. Choi TW, Kim HC, Lee JH, Yu SJ, Kang B, Hur S, et al. The safety and clinical outcomes of chemoembolization in child-pugh class C patients with hepatocellular carcinomas. Korean J Radiol. 2015; 16:1283–1293. PMID: 26576118.
Article8. Liu PH, Hsu CY, Lee YH, Hsia CY, Huang YH, Su CW, et al. When to perform surgical resection or radiofrequency ablation for early hepatocellular carcinoma?: a nomogram-guided treatment strategy. Medicine (Baltimore). 2015; 94:e1808. PMID: 26512576.9. Wang X, Hu Y, Ren M, Lu X, Lu G, He S. Efficacy and safety of radiofrequency ablation combined with transcatheter arterial chemoembolization for hepatocellular carcinomas compared with radiofrequency ablation alone: a time-to-event meta-analysis. Korean J Radiol. 2016; 17:93–102. PMID: 26798221.
Article10. Bertrand J, Caillol F, Borentain P, Raoul JL, Heyries L, Bories E, et al. Percutaneous hepatic radiofrequency for hepatocellular carcinoma: results and outcome of 46 patients. Hepat Med. 2015; 7:21–27. PMID: 26056497.
Article11. Abdelaziz AO, Abdelmaksoud AH, Nabeel MM, Shousha HI, Cordie AA, Mahmoud ShH, et al. Transarterial chemoembolization combined with either radiofrequency or microwave ablation in management of hepatocellular carcinoma. Asian Pac J Cancer Prev. 2017; 18:189–194. PMID: 28240516.12. Xu Y, Shen Q, Wang N, Liu P, Wu P, Peng Z, et al. Percutaneous microwave ablation of 5-6 cm unresectable hepatocellular carcinoma: local efficacy and long-term outcomes. Int J Hyperthermia. 2017; 33:247–254.13. Si ZM, Wang GZ, Qian S, Qu XD, Yan ZP, Liu R, et al. Combination therapies in the management of large (≥ 5 cm) hepatocellular carcinoma: microwave ablation immediately followed by transarterial chemoembolization. J Vasc Interv Radiol. 2016; 27:1577–1583. PMID: 27103146.
Article14. Bruix J, Sherman M. American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology. 2011; 53:1020–1022. PMID: 21374666.
Article15. Choe WH, Kim YJ, Park HS, Park SW, Kim JH, Kwon SY. Short-term interval combined chemoembolization and radiofrequency ablation for hepatocellular carcinoma. World J Gastroenterol. 2014; 20:12588–12594. PMID: 25253962.
Article16. Kang HJ, Kim YI, Kim HC, Jae HJ, Hur S, Chung JW. Does establishing a safety margin reduce local recurrence in subsegmental transarterial chemoembolization for small nodular hepatocellular carcinomas? Korean J Radiol. 2015; 16:1068–1078. PMID: 26357501.
Article17. Lee EW, Alanis L, Cho SK, Saab S. Yttrium-90 selective internal radiation therapy with glass microspheres for hepatocellular carcinoma: current and updated literature review. Korean J Radiol. 2016; 17:472–488. PMID: 27390539.
Article18. Lencioni R, Montal R, Torres F, Park JW, Decaens T, Raoul JL, et al. Objective response by mRECIST as a predictor and potential surrogate end-point of overall survival in advanced HCC. J Hepatol. 2017; 66:1166–1172. PMID: 28131794.
Article19. Zhu ZX, Liao MH, Wang XX, Huang JW. Transcatheter arterial chemoembolization plus 131i-labelled metuximab versus transcatheter arterial chemoembolization alone in intermediate/advanced stage hepatocellular carcinoma: a systematic review and meta-analysis. Korean J Radiol. 2016; 17:882–892. PMID: 27833404.20. Lahat E, Eshkenazy R, Zendel A, Zakai BB, Maor M, Dreznik Y, et al. Complications after percutaneous ablation of liver tumors: a systematic review. Hepatobiliary Surg Nutr. 2014; 3:317–323. PMID: 25392844.21. Schneeweiß S, Horger M, Ketelsen D, Ioanoviciu SD. [Complications after TACE in HCC - complications after transarterial chemoembolization (TACE) in hepatocellular carcinoma]. Rofo. 2015; 187:79–82. PMID: 25629286.22. Schlachterman A, Craft WW Jr, Hilgenfeldt E, Mitra A, Cabrera R. Current and future treatments for hepatocellular carcinoma. World J Gastroenterol. 2015; 21:8478–8491. PMID: 26229392.
Article23. Massani M, Stecca T, Ruffolo C, Bassi N. Should we routinely use DEBTACE for unresectable HCC? cTACE versus DEBTACE: a single-center survival analysis. Updates Surg. 2017; 69:67–73. PMID: 28097502.
Article24. Liu YS, Ou MC, Tsai YS, Lin XZ, Wang CK, Tsai HM, et al. Transarterial chemoembolization using gelatin sponges or microspheres plus lipiodol-doxorubicin versus doxorubicin-loaded beads for the treatment of hepatocellular carcinoma. Korean J Radiol. 2015; 16:125–132. PMID: 25598680.
Article25. Wang W, Shi J, Xie WF. Transarterial chemoembolization in combination with percutaneous ablation therapy in unresectable hepatocellular carcinoma: a meta-analysis. Liver Int. 2010; 30:741–749. PMID: 20331507.
Article26. Zhao M, Wang JP, Pan CC, Li W, Huang ZL, Zhang L, et al. CT-guided radiofrequency ablation after with transarterial chemoembolization in treating unresectable hepatocellular carcinoma with long overall survival improvement. Eur J Radiol. 2012; 81:2717–2725. PMID: 22245655.
Article27. Xu LF, Sun HL, Chen YT, Ni JY, Chen D, Luo JH, et al. Large primary hepatocellular carcinoma: transarterial chemoembolization monotherapy versus combined transarterial chemoembolization-percutaneous microwave coagulation therapy. J Gastroenterol Hepatol. 2013; 28:456–463. PMID: 23216261.
Article28. Lucchina N, Tsetis D, Ierardi AM, Giorlando F, Macchi E, Kehagias E, et al. Current role of microwave ablation in the treatment of small hepatocellular carcinomas. Ann Gastroenterol. 2016; 29:460–465. PMID: 27708511.
Article29. Fong ZV, Palazzo F, Needleman L, Brown DB, Eschelman DJ, Chojnacki KA, et al. Combined hepatic arterial embolization and hepatic ablation for unresectable colorectal metastases to the liver. Am Surg. 2012; 78:1243–1248. PMID: 23089443.30. Ni JY, Sun HL, Chen YT, Luo JH, Chen D, Jiang XY, et al. Prognostic factors for survival after transarterial chemoembolization combined with microwave ablation for hepatocellular carcinoma. World J Gastroenterol. 2014; 20:17483–17490. PMID: 25516662.
Article31. Kim JW, Kim JH, Won HJ, Shin YM, Yoon HK, Sung KB, et al. Hepatocellular carcinomas 2-3 cm in diameter: transarterial chemoembolization plus radiofrequency ablation vs. radiofrequency ablation alone. Eur J Radiol. 2012; 81:e189–e193. PMID: 21353417.32. Sun AX, Cheng ZL, Wu PP, Sheng YH, Qu XJ, Lu W, et al. Clinical outcome of medium-sized hepatocellular carcinoma treated with microwave ablation. World J Gastroenterol. 2015; 21:2997–3004. PMID: 25780298.
Article33. Salvalaggio PR, Felga GE, Alves JA, Meirelles RF Jr, Almeida MD, de Rezende MB. Response to transarterial chemoembolization in candidates with hepatocellular carcinoma within Milan criteria does not predict post-transplant disease-free survival. Transplant Proc. 2014; 46:1799–1802. PMID: 25131040.
Article34. Yin X, Zhang L, Wang YH, Zhang BH, Gan YH, Ge NL, et al. Transcatheter arterial chemoembolization combined with radiofrequency ablation delays tumor progression and prolongs overall survival in patients with intermediate (BCLC B) hepatocellular carcinoma. BMC Cancer. 2014; 14:849. PMID: 25409554.
Article35. Jin YJ, Lee JW. Therapeutic priorities for solitary large hepatocellular carcinoma in a hepatitis B virus endemic area; an analysis of a nationwide cancer registry database. J Surg Oncol. 2017; 115:407–416. PMID: 28008620.
Article36. Kawaguchi T, Ohkawa K, Imanaka K, Tamai C, Kawada N, Ikezawa K, et al. Lipiodol accumulation and transarterial chemoembolization efficacy for HCC patients. Hepatogastroenterology. 2012; 59:219–223. PMID: 22260832.
Article37. Leung U, Kuk D, D'Angelica MI, Kingham TP, Allen PJ, DeMatteo RP, et al. Long-term outcomes following microwave ablation for liver malignancies. Br J Surg. 2015; 102:85–91. PMID: 25296639.
Article38. Jianyong L, Lunan Y, Wentao W, Yong Z, Bo L, Tianfu W, et al. Barcelona clinic liver cancer stage B hepatocellular carcinoma: transarterial chemoembolization or hepatic resection? Medicine (Baltimore). 2014; 93:e180. PMID: 25474433.39. Liu PH, Su CW, Hsu CY, Hsia CY, Lee YH, Huang YH, et al. Solitary large hepatocellular carcinoma: staging and treatment strategy. PLoS One. 2016; 11:e0155588. PMID: 27176037.
Article40. Kim JH, Shim JH, Lee HC, Sung KB, Ko HK, Ko GY, et al. New intermediate-stage subclassification for patients with hepatocellular carcinoma treated with transarterial chemoembolization. Liver Int. 2017; 37:1861–1868. PMID: 28581250.
Article41. Peng ZW, Zhang YJ, Chen MS, Xu L, Liang HH, Lin XJ, et al. Radiofrequency ablation with or without transcatheter arterial chemoembolization in the treatment of hepatocellular carcinoma: a prospective randomized trial. J Clin Oncol. 2013; 31:426–432. PMID: 23269991.
Article42. Yamakado K, Miyayama S, Hirota S, Mizunuma K, Nakamura K, Inaba Y, et al. Subgrouping of intermediate-stage (BCLC stage B) hepatocellular carcinoma based on tumor number and size and Child-Pugh grade correlated with prognosis after transarterial chemoembolization. Jpn J Radiol. 2014; 32:260–265. PMID: 24615165.
Article43. Zhong JH, Rodríguez AC, Ke Y, Wang YY, Wang L, Li LQ. Hepatic resection as a safe and effective treatment for hepatocellular carcinoma involving a single large tumor, multiple tumors, or macrovascular invasion. Medicine (Baltimore). 2015; 94:e396. PMID: 25621684.
Article44. Dong ZR, Zhang PF, Wang CH, Zhang C, Cai JB, Shi GM, et al. Postoperative adjuvant transcatheter arterial chemoembolization for resectable multiple hepatocellular carcinoma beyond the Milan criteria: a retrospective analysis. Am J Cancer Res. 2014; 5:450–457. PMID: 25628953.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Efficacy of Hepatic Arterial Infusion Chemotherapy and Radiofrequency Ablation against Hepatocellular Carcinoma Refractory to Transarterial Chemoembolization and Vascular Variation: A Case Study
- The Role of Combination of Transarterial Chemoebolization and Radiofrequency Ablation for Hepatocellular Carcinoma Treatment
- Complications Related to Transarterial Treatment of Hepatocellular Carcinoma: A Comprehensive Review
- Transarterial Chemoembolization in Patients with Hepatocellular Carcinoma and Extrahepatic Metastasis
- Comparison of surgical resection versus transarterial chemoembolization with additional radiation therapy in patients with hepatocellular carcinoma with portal vein invasion
