A Case of Intravitreal Dexamethasone Implantation in a Patient with Vogt-Koyanagi-Harada Disease
- Affiliations
-
- 1Department of Ophthalmology, Jeju National University Hospital, Jeju National University School of Medicine, Jeju, Korea. righthanded8282@gmail.com
- KMID: 2403815
- DOI: http://doi.org/10.3341/jkos.2018.59.2.190
Abstract
- PURPOSE
To report a case of Vogt-Koyanagi-Harada (VKH) disease with chronic recurrence, which was treated with intravitreal dexamethasone implantation.
CASE SUMMARY
A 39-year-old female presented with decreased visual acuities in both eyes accompanied by headaches and tinnitus the previous week. On fundus examination and optical coherence tomography, multiple serous retinal detachments with subretinal septa were observed in both eyes, and she was diagnosed with VKH disease. After undergoing high dose intravenous steroid therapy at another hospital, she was treated with oral prednisolone and immunosuppressant drugs. However, she showed frequent recurrences, and also complained of side effects from prolonged systemic steroids. We then performed intravitreal injections of dexamethasone implants in both eyes at 3-week intervals. One month following the injections, the inflammations in the anterior chamber and vitreous opacities were improved. Until the last visit at 6 months after the injection, there was no significant recurrence of inflammation, although oral prednisolone had been tapered.
CONCLUSIONS
In VKH disease, intravitreal dexamethasone implantation may be an effective treatment option if chronic recurrence occurs, despite systemic steroid and immunosuppressant therapy or sustained treatment being difficult to maintain because of side effects.
MeSH Terms
Figure
-

Figure 1. Fundus color photographs (A, B) and optical coherence tomography (OCT) images (C, D) at the first visit. Fundus color photographs of right (A) and left (B) eye showed multiple serous retinal detachments. OCT images of right (C) and left (D) eye revealed massive subretinal exudative fluid and subretinal septa. Long thin white arrows indicate OCT scan direction.
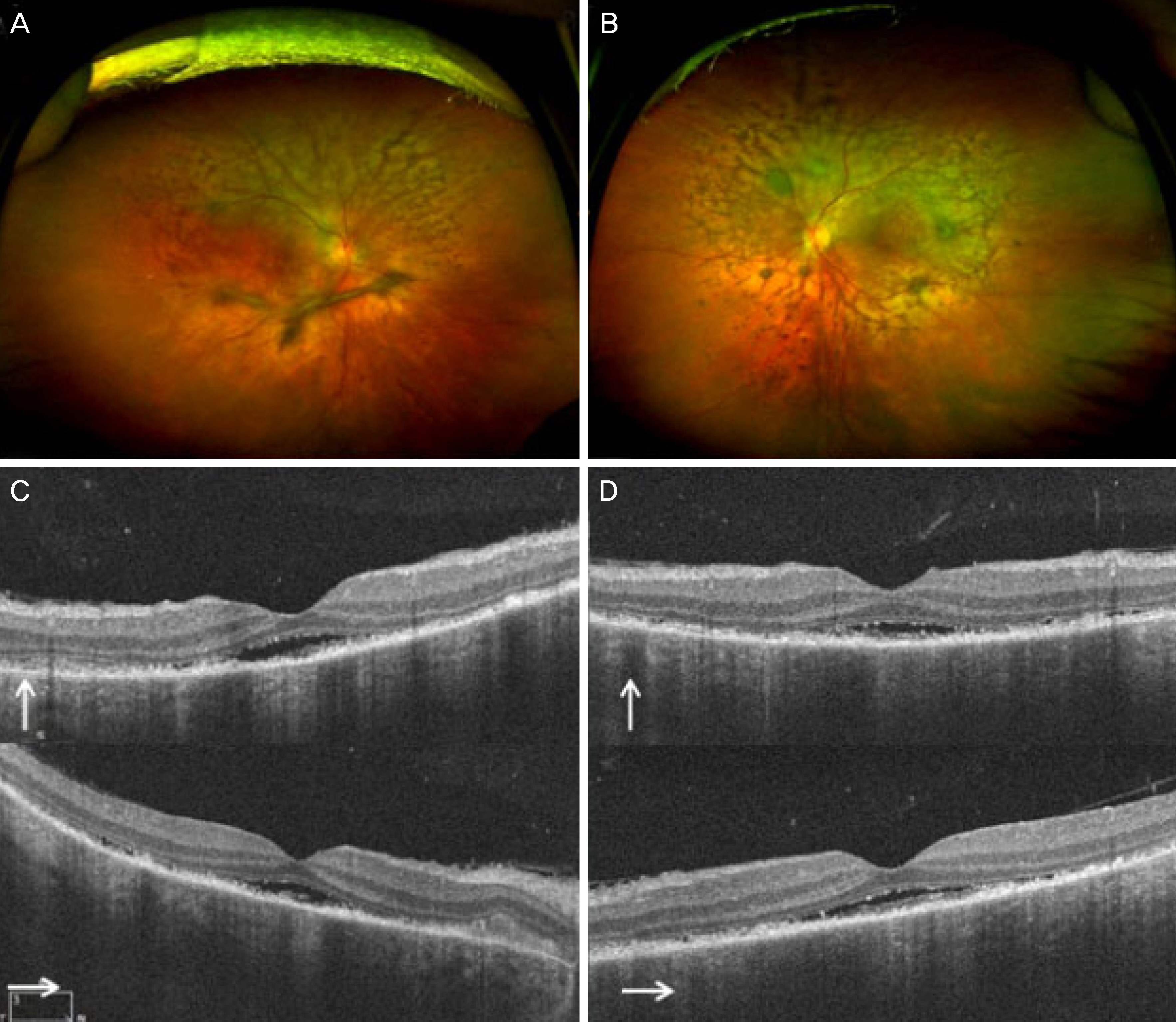
Figure 2. Fundus color photographs (A, B) and optical coherence tomography (OCT) images (C, D) after intravenous steroid pulse therapy following high dose oral steroid. (A, B) Sunset glow fundus with retinal pigment epithelium clumping are shown. (C, D) The serous retinal detachment is greatly improved but shallow subretinal fluid still remained beneath the fovea. Long thin white arrows indicate OCT scan direction.
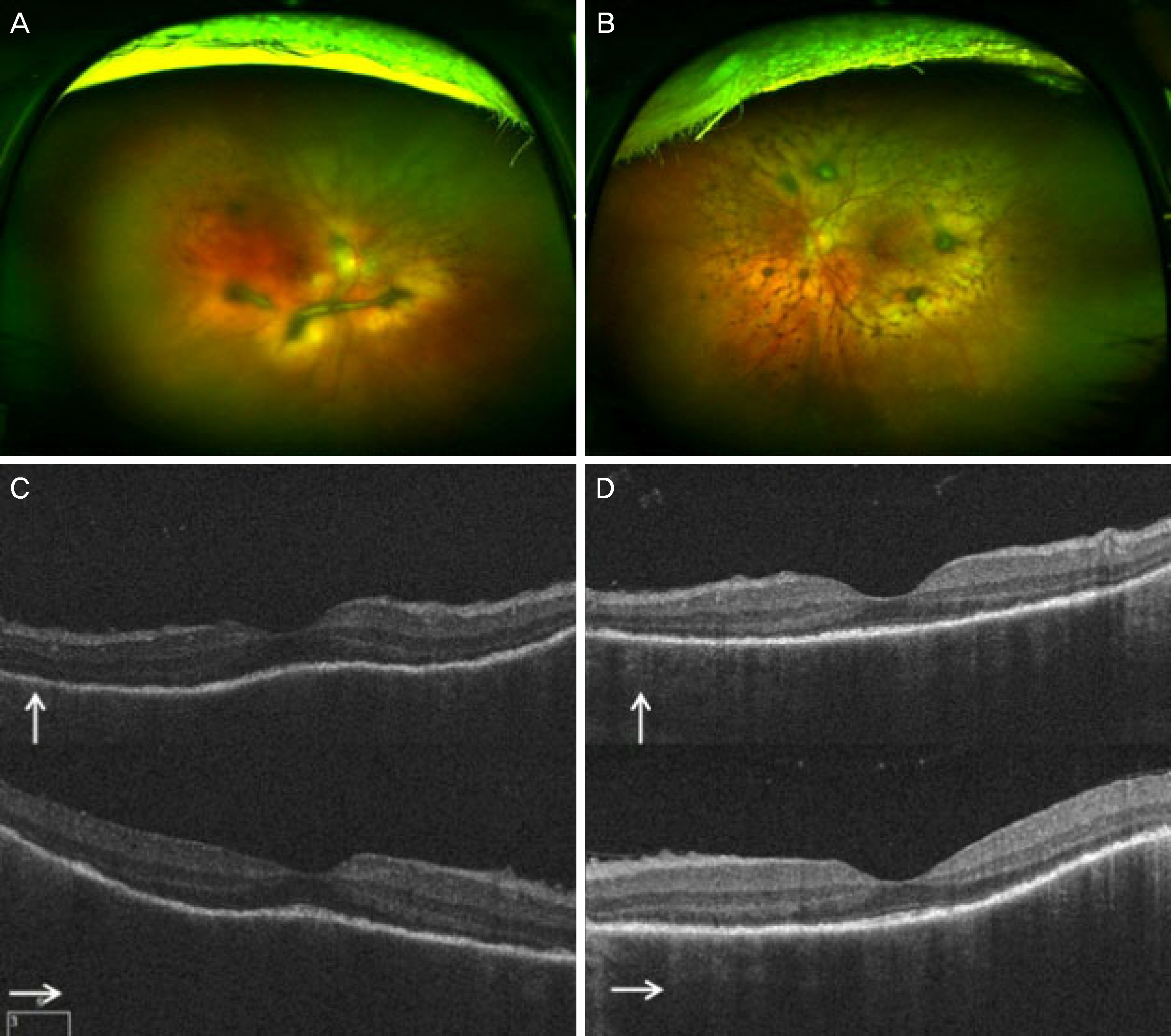
Figure 3. Fundus color photographs (A, B) and optical coherence tomography (OCT) images (C, D) before intravitreal dexamethasone implant injection. (A, B) Severe vitreous opacities are present. (C, D) Although subretinal fluid was absorbed, vitreous opacities with undulation of retinal pigment epithelium are shown and choroidal thickness increased. Long thin white arrows indicate OCT scan direction.
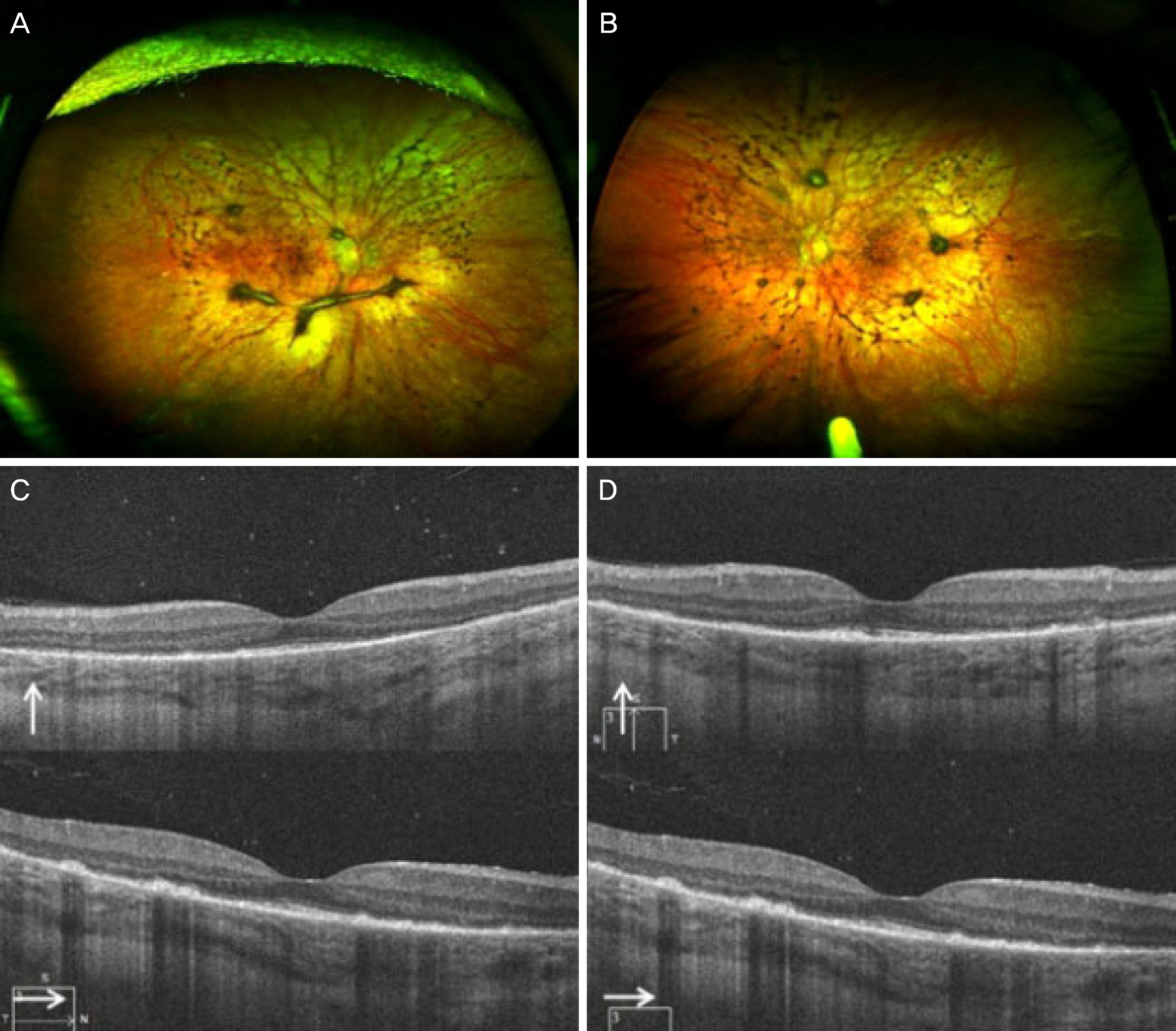
Figure 4. Fundus color photographs (A, B) and optical coherence tomography (OCT) images (C, D) at 1 month after intravitreal dexamethasone implant injection. (A, B) The vitreous opacities diminished. (C, D) The vitreous opacities with retinal pigment epithelium undulation were improved and choroidal thickness decreased. Long thin white arrows indicate OCT scan direction.
Reference
-
References
1. Sugiura S. Vogt-Koyanagi-Harada disease. Jpn J Ophthalmol. 1978; 22:9–35.
Article2. Sakata VM, da Silva FT, Hirata CE, et al. Diagnosis and abdominal of Vogt-Koyanagi-Harada disease. Autoimmun Rev. 2014; 13:550–5.3. Urzua CA, Velasquez V, Sabat P, et al. Earlier immunomodulatory treatment is associated with better visual outcomes in a subset of patients with Vogt–Koyanagi–Harada disease. Acta Ophthalmol. 2015; 93:e475–80.
Article4. González-Delgado M, González C, Blázquez JI, et al. Intravenous immunoglobulin therapy in Vogt-Koyanagi-Harada syndrome. Neurologia. 2004; 19:401–3.5. Errera MH, Fardeau C, Cohen D, et al. Effect of the duration of abdominal therapy on the clinical features of recurrent episodes in Vogt–Koyanagi–Harada disease. Acta Ophthalmol. 2011; 89:e357–66.6. Boyer DS, Yoon YH, Belfort R Jr, et al. Three-year, randomized, sham-controlled trial of dexamethasone intravtreal implant in abdominals with diabetic macular edema. Ophthalmology. 2014; 121:1904–14.7. Haller JA, Bandello F, Belford R Jr, et al. Randomized, sham-abdominalled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology. 2010; 117:1134–46.e3.8. Myung JS, Aaker GD, Kiss S. Treatment of noninfectious posterior uveitis with dexamethasone intravitreal implant. Clin Ophthalmol. 2010; 4:1423–6.9. Rao NA, Sukavatcharin S, Tsai JH. Vogt-Koyanagi-Harada disease diagnostic criteria. Int Ophthalmol. 2007; 27:195–9.
Article10. Moorthy RS, Inomata H, Rao NA. Vogt–Koyanagi–Harada syndrome. Surv Ophthalmol. 1995; 39:265–92.
Article11. Carnahan MC, Goldstein DA. Ocular complications of topical, periocular, and systemic corticosteroid. Curr Opin Ophthalmol. 2000; 11:478–83.12. Lowder C, Belford R, Lightman S, et al. Dexamethasone abdominal implant for noninfectious intermediate or posterior uveitis. Arch Ophthalmol. 2011; 129:545–53.13. Latronico ME, Rigante D, Caso F, et al. Bilateral dexamethasone intravitreal implant in a young patient with Vogt-Koyanagi-Harada disease and refractory uveitis. Clin Rheumatol. 2015; 34:1145–8.
Article14. Ryder SJ, Iannetta D, Bhaleeya SD, Kiss S. Efficacy and abdominal of bilateral sustained-release dexamethasone intravitreal implants for the treatment of noninfectious posterior uveitis and macular edema secondary to retinal vein occlusion. Clin Ophthalmol. 2015; 9:1109–16.15. Bakri SJ, Risco M, Edwards AO, Pulido JS. Bilateral simultaneous intravitreal injections in the office setting. Am J Ophthalmol. 2009; 148:66–9.e1.
Article16. Abu-Yaghi NE, Shokry AN, Abu-Sbeit RH. Bilateral same-session intravitreal injections of anti-vascular endothelial growth factors. Int J Ophthalmol. 2014; 7:1017–21.17. Woo SJ, Han JM, Ahn J, et al. Bilateral same-day intravitreal abdominals using a single vial and molecular bacterial screening for safety surveillance. Retina. 2012; 32:667–71.
