Conservative Treatment of Mid-Clavicle Fractures
- Affiliations
-
- 1Deparment of Orthopaedic Surgery, Korea University College of Medicine, Seoul, Korea. drshoulder@korea.ac.kr
- KMID: 2402711
- DOI: http://doi.org/10.12671/jkfs.2018.31.1.22
Abstract
- Clavicle fractures are very common injuries in adults and children and the majority of these fractures occur in the midshaft. Traditionally, mid-clavicle fractures have been treated with conservative methods and the clinical outcomes of this method are believed to be excellent. On the other hand, recent studies have shown that the clinical results of severe comminuted or markedly displaced fractures after conservative management were not as favorable as previously described. Despite these concerns, the conservative treatment of mid-clavicle fractures is still an efficient method, which can be applied to all patients as a primary care. This review focuses on the proper indication, technique, and limitations of conservative treatment of mid-clavicle fractures.
Keyword
Figure
-
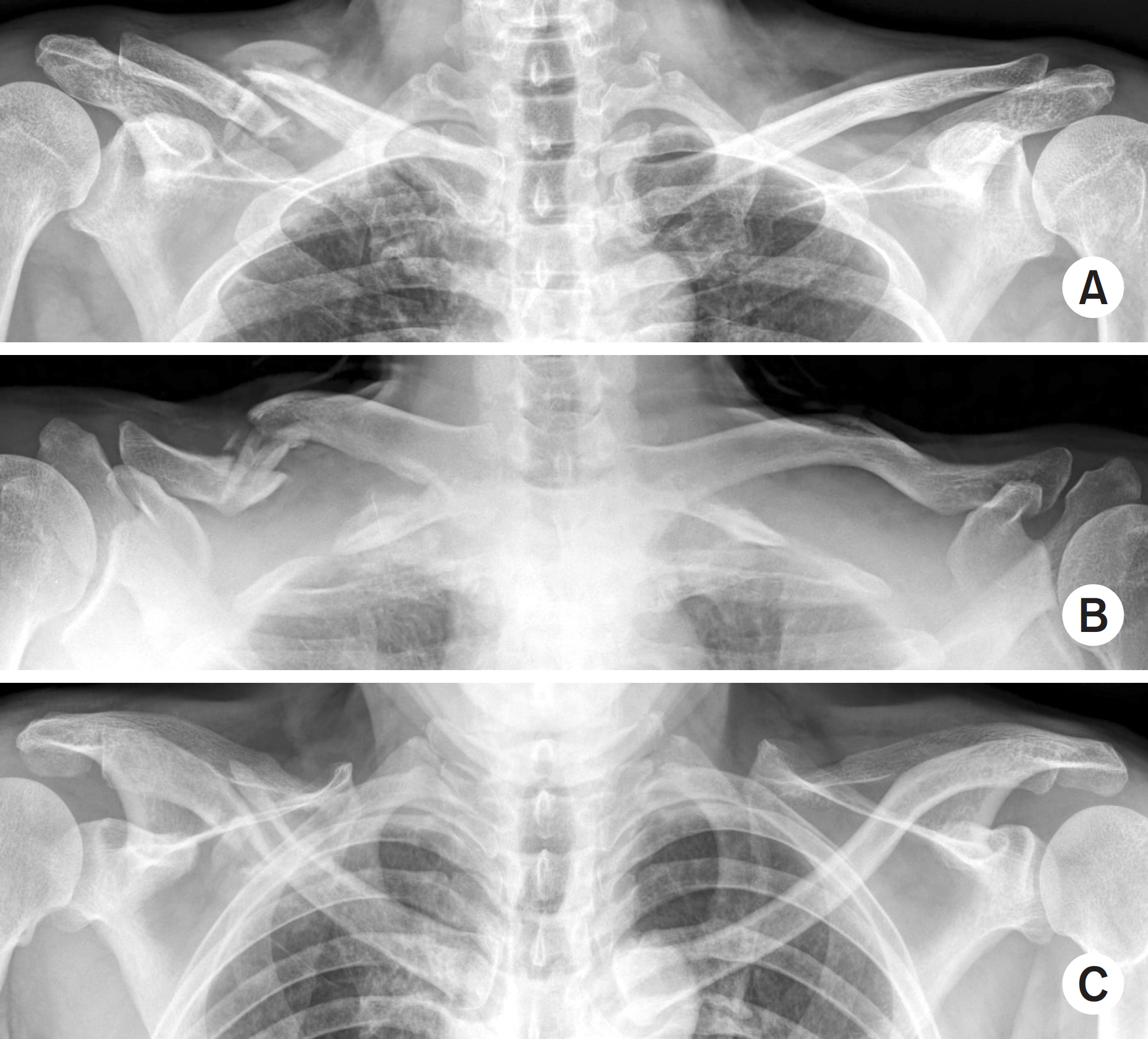
Fig. 1. Plain radiographs to evaluate mid-clavicle fractures. (A) Anterior-posterior projection: shortening of the clavicle and drooping of the shoulder girdle is prominent in this view. (B) Caudal tilting view: Anterior-posterior displacement is prominent in this view. (C) Cephalad tilting view: S shape of clavicle is prominent in this view.
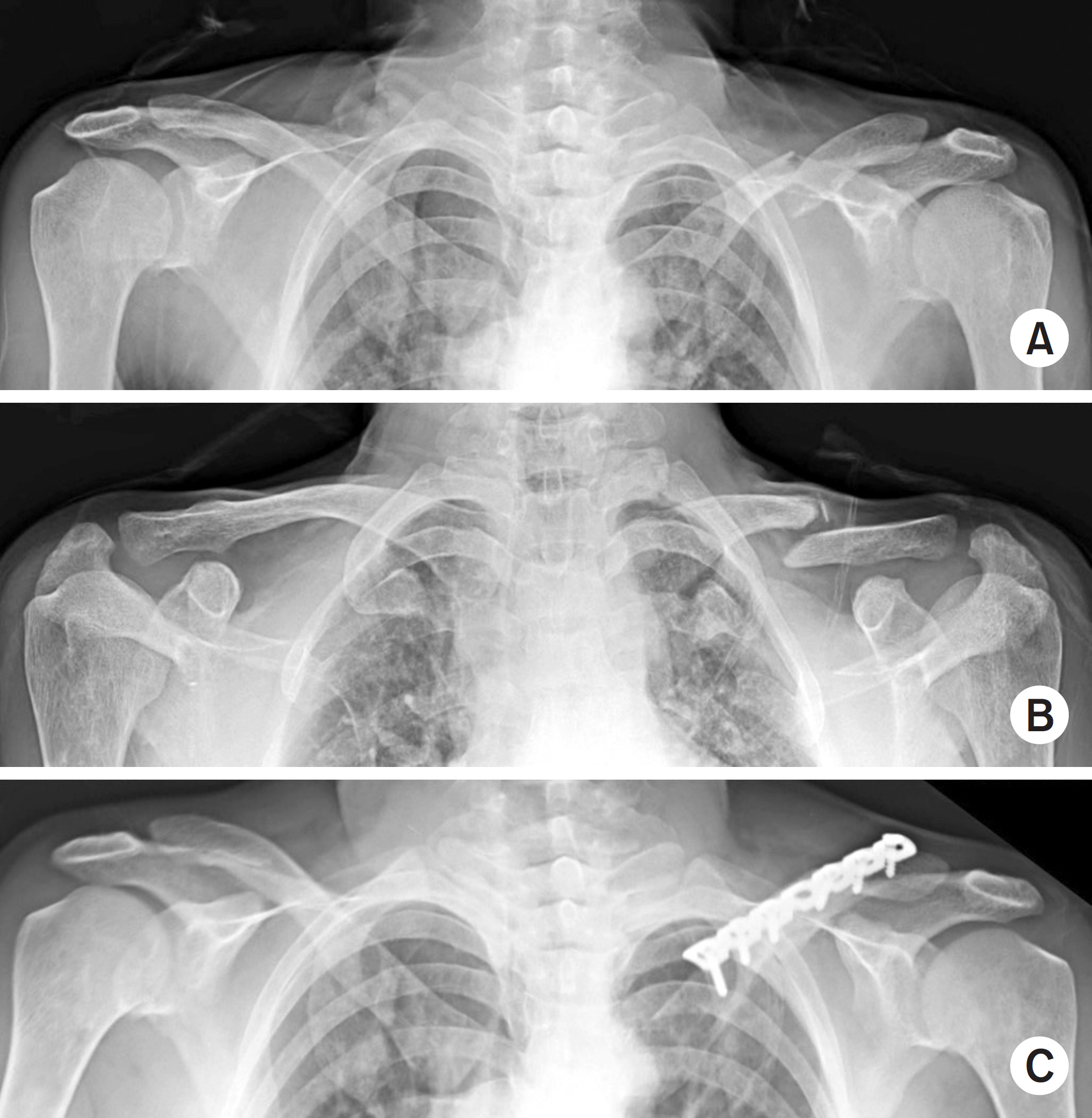
Fig. 2. A 47-year-old woman suffered a left mid-clavicle fracture. (A) Initial anteroposterior radiograph shows minimal cortical contact between the fracture fragments. (B) There is no evidence of fracture healing 6 months after conservative treatment. (C) Plain radiographs taken 1 year after plate fixation and bone graft shows solid bone union.

Fig. 3. An 82-year-old woman suffered a left clavicle fracture. (A) Non-union was observed after conservative treatment 9 months after the initial trauma. (B) Although her clavicle fracture had not healed, she had an acceptable appearance. (C) She also shows good shoulder function (She permitted printing her face and photos in this journal.).
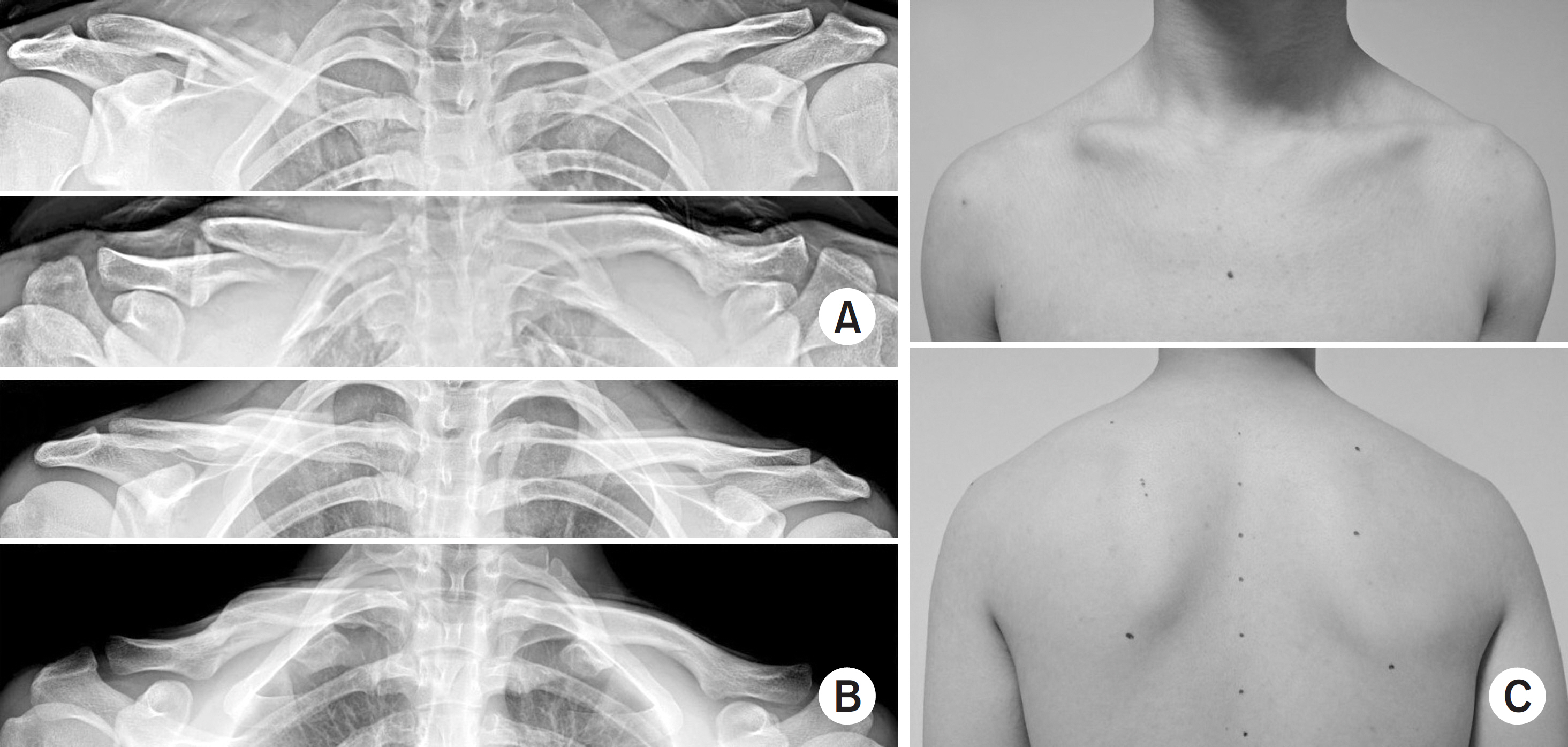
Fig. 4. A 21-year-old man suffered a right clavicle fracture. (A) Initial radiographs shows some cortical contact between the fracture fragments but shortening of the clavicle is visible. (B) Plain radiographs taken 1 year after trauma shows shortening of the clavicle and different versions of glenoid fossa. (C) One year after trauma, his clinical photos shows prominent fracture site and drooping of the right shoulder girdle. He was not satisfied with the outcome.
Reference
-
References
1. Nordqvist A, Petersson CJ, Redlund-Johnell I. Mid-clavicle fractures in adults: end result study after conservative treatment. J Orthop Trauma. 12:572–576. 1998.
Article2. Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br. 80:476–484. 1998.3. Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology of clavicle fractures. J Shoulder Elbow Surg. 11:452–456. 2002.
Article4. Neer CS. Fractures of the clavicle. Rockwood CA, Green DP, editors. Fractures in adults. 2nd ed.Philadelphia, JB Lippincott Company: 707–713;1984.5. Robinson CM, Cairns DA. Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am. 86:778–782. 2004.
Article6. Throckmorton T, Kuhn JE. Fractures of the medial end of the clavicle. J Shoulder Elbow Surg. 16:49–54. 2007.
Article7. Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am. 86:1359–1365. 2004.
Article8. Andermahr J, Jubel A, Elsner A, et al. Malunion of the clavicle causes significant glenoid malposition: a quantitative anatomic investigation. Surg Radiol Anat. 8:447–456. 2006.
Article9. Lazarides S, Zafiropoulos G. Conservative treatment of fractures at the middle third of the clavicle: the relevance of shortening and clinical outcome. J Shoulder Elbow Surg. 15:191–194. 2006.
Article10. McKee MD, Pedersen EM, Jones C, et al. Deficits following nonoperative treatment of displaced midshaft clavicular fractures. J Bone Joint Surg Am. 88:35–40. 2006.
Article11. Postacchini R, Gumina S, Farsetti P, Postacchini F. Long-term results of conservative management of midshaft clavicle fracture. Int Orthop. 34:731–736. 2010.
Article12. Robinson CM, Goudie EB, Murray IR, Jenkins PJ, Ahktar MA, Read EO. Open reduction and plate fixation versus nonoperative treatment for displaced midshaft clavicular fractures: a multicenter, randomized, controlled trial. J Bone Joint Surg Am. 95:1576–1584. 2013.13. Heuer HJ, Boykin RE, Petit CJ, Hardt J, Millett PJ. Decision-making in the treatment of diaphyseal clavicle fractures: is there agreement among surgeons? Results of a survey on surgeons' treatment preferences. J Shoulder Elbow Surg. 23:e23–e33. 2014.14. Ban I, Nowak J, Virtanen K, Troelsen A. Overtreatment of displaced midshaft clavicle fractures. Acta Orthop. 87:541–545. 2016.
Article15. Lenza M, Faloppa F. Conservative interventions for treating middle third clavicle fractures in adolescents and adults. Cochrane Database Syst Rev. 12:CD007121. 2016.
Article16. Andersen K, Jensen PO, Lauritzen J. Treatment of clavicular fractures. Figure-of-eight bandage versus a simple sling. Acta Orthop Scand. 58:71–74. 1987.17. Rowe CR. An atlas of anatomy and treatment of midclavicular fractures. Clin Orthop Relat Res. 58:29–42. 1968.18. Neer CS 2nd. Nonunion of the clavicle. J Am Med Assoc. 172:1006–1011. 1960.
Article19. Zlowodzki M, Zelle BA, Cole PA, Jeray K, McKee MD. Evidence-Based Orthopaedic Trauma Working Group. Treatment of acute midshaft clavicle fractures: systematic review of 2144 fractures: on behalf of the Evidence-Based Orthopaedic Trauma Working Group. J Orthop Trauma. 19:504–507. 2005.20. Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J Bone Joint Surg Am. 89:1–10. 2007.21. Hill JM, McGuire MH, Crosby LA. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br. 79:537–539. 1997.
Article22. Matsumura N, Ikegami H, Nakamichi N, et al. Effect of shortening deformity of the clavicle on scapular kinematics: a cadaveric study. Am J Sports Med. 38:1000–1006. 2010.23. Ahrens PM, Garlick NI, Barber J, Tims EM. Clavicle Trial Collaborative Group. The clavicle trial: a multicenter randomized controlled trial comparing operative with nonoperative treatment of displaced midshaft clavicle fractures. J Bone Joint Surg Am. 99:1345–1354. 2017.24. Daniilidis K, Raschke MJ, Vogt B, et al. Comparison between conservative and surgical treatment of midshaft clavicle fractures: outcome of 151 cases. Technol Health Care. 21:143–147. 2013.
Article25. van der Ven Denise JC, Timmers TK, Flikweert PE, Van Ijseldijk AL, van Olden GD. Plate fixation versus conservative treatment of displaced midshaft clavicle fractures: functional outcome and patients'satisfaction during a mean follow-up of 5 years. Injury. 46:2223–2229. 2015.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current concepts in the treatment of midshaft clavicle fractures in adults
- Current Concepts for Classification and Treatment of Distal Clavicle Fractures
- Periprosthetic Clavicle Shaft Fracture After Treatment of Type V Distal Clavicle Fracture Using a Hook Plate: A Report of Two Cases
- The Different Treatment Methods for Segmental Fractures of the Clavicle: Cases Report
- Comparison of Results Between Immediate Fixation Group and Delayed Reconstruction Group in Displaced Mid-shaft Fractures of the Clavicle
