Kosin Med J.
2017 Dec;32(2):233-239. 10.7180/kmj.2017.32.2.233.
IgG4-Related Disease with lymphadenopathy Presenting as a Cervical lymph node enlargement
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Konyang University, Daejeon, Korea. dycho@kyuh.ac.kr
- 2Department of Pathology, College of Medicine, Konyang University, Daejeon, Korea.
- KMID: 2400267
- DOI: http://doi.org/10.7180/kmj.2017.32.2.233
Abstract
- During the course of evaluation and management of neck masses, consideration for Immunoglobulin G4-related disease (IgG4-RD) should be given. IgG4-RD is relatively a new growing entity of immune-mediated origin, characterized by a mass-forming lesion, the infiltration of IgG4-positive plasma cells and occasionally elevated serum IgG4. The most common manifestations are parotid and lacrimal swelling, lymphadenopathy and autoimmune pancreatitis. A previously healthy 72-year-old man was referred to our clinic with a 2-month history of left cervical lymph node enlargement without systemic manifestations . A cervical lymph node biopsy was planned because of elevated serum IgG4 levels. Pathological findings showed prominent infiltration of IgG4-postive plasma cells in the lymph node. After steroid therapy, a computed tomography scan revealed a decrease in the cervical lymph node size. This case illustrates the importance of including IgG4-RD in the differential diagnosis of a cervical lymph node enlargement.
Keyword
MeSH Terms
Figure
-

Fig. 1 Fig. 1A. Initial neck CT(Computed Tomography) showed multiple cervical lymph node enlargement, Fig. 1B. Post-steroid treatment image (The size of the cervical lymph node decreased after 8 month steroid trial)
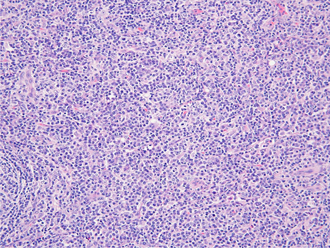
Fig. 2 Histological findings in Lt. cervical LN biopsy specimen, H&E staining ×200
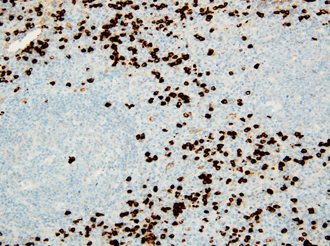
Fig. 3 Histological findings in Lt. cervical LN biopsy specimen, Interfollicular and perisinusoidal infiltration of small and large lymphocytes, admixed atrophic and hyperplastic germinal centers, large numbers of plasma cells showing IgG4 immunoreactivities (>100/HPF), Immunohistochemicalstaining × 200
Reference
-
1. Habermann TM, Steensma DP. Lymphadenopathy. Mayo Clin Proc. 2000; 75:723–732.
Article2. Kamisawa T, Zen Y, Pillai S, Stone JH. IgG4-related disease. Lancet. 2015; 385:1460–1471.
Article3. Khosroshahi A, Stone JH. Treatment approaches to IgG4-related systemic disease. Curr Opin Rheumatol. 2011; 23:67–71.
Article4. Nizar AH, Toubi E. IgG4-related disease: case report and literature review. Auto Immun Highlights. 2015; 6:7–15.
Article5. Zen Y, Nakanuma Y. IgG4-related disease: a cross-sectional study of 114 cases. Am J Surg Pathol. 2010; 34:1812–1819.6. Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, et al. A novel clinical entity, IgG4-related disease (IgG4RD): general concept and details. Mod Rheumatol. 2012; 22:1–14.
Article7. Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012; 366:539–551.
Article8. Ghably JG, Borthwick T, O'Neil TJ, Youngberg GA, Datta AA, Krishnaswamy G. IgG4-related disease: a primer on diagnosis and management. Ann Allergy Asthma Immunol. 2015; 114:447–454.
Article9. Cornell LD. IgG4-related kidney disease. Semin Diagn Pathol. 2012; 29:245–250.
Article10. Shimosegawa T, Chari ST, Frulloni L, Kamisawa T, Kawa S, Mino-kenudson M, et al. International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology. Pancreas. 2011; 40:352–358.
Article11. Khosroshahi A, Bloch DB, Deshpande V, Stone JH. Rituximab therapy leads to rapid decline of serum IgG4 levels and prompt clinical improvement in IgG4-related systemic disease. Arthritis Rheum. 2010; 62:1755–1762.
Article12. Cheuk W, Chan JK. Lymphadenopathy of IgG4-related disease: an underdiagnosed and overdiagnosed entity. Semin Diagn Pathol. 2012; 29:226–234.
Article13. Kamisawa T, Nakajima H, Egawa N, Funata N, Tsuruta K, Okamoto A. IgG4-related sclerosing disease incorporating sclerosing pancreatitis, cholangitis, sialadenitis and retroperitoneal fibrosis with lymphadenopathy. Pancreatology. 2006; 6:132–137.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mikulicz's Disease with Progressively Transformed Germinal Centers-type Immunoglobulin G4-related Lymphadenopathy Mimicking Sjogren's Syndrome
- Ultrasonographic Evaluation of Cervical Lymph Nodes
- MRI Findings of Cervical Lymphadenopathy: Preliminary Study
- A Case of Rosai-Dorfman Disease Presented with Neck Mass
- CD68 Positive Histiocytic Necrotizing Lymphadenitis
